View full-text in Spanish
Abstract
Background:
The best scientific evidence is required to design effective Non-pharmaceutical interventions to help policymakers to contain COVID-19.
Aim:
To describe which Non-pharmaceutical interventions used different countries and a when they use them. It also explores how Non-pharmaceutical interventions impact the number of cases, the mortality, and the capacity of health systems.
Methods:
We consulted eight web pages of transnational organizations, 17 of international media, 99 of government institutions in the 19 countries included, and besides, we included nine studies (out of 34 identified) that met inclusion criteria.
Result:
Some countries are focused on establishing travel restrictions, isolation of identified cases, and high-risk people. Others have a combination of mandatory quarantine and other drastic social distancing measures. The timing to implement the interventions varied from the first fifteen days after detecting the first case to more than 30 days. The effectiveness of isolated non-pharmaceutical interventions may be limited, but combined interventions have shown to be effective in reducing the transmissibility of the disease, the collapse of health care services, and mortality. When the number of new cases has been controlled, it is necessary to maintain social distancing measures, self-isolation, and contact tracing for several months. The policy decision-making in this time should be aimed to optimize the opportunities of saving lives, reducing the collapse of health services, and minimizing the economic and social impact over the general population, but principally over the most vulnerable. The timing of implementing and lifting interventions could have a substantial effect on those objectives.
Keywords: COVID-19, Coronavirus, Review, Public Health, Quarantine, Health Impact Assessment
Remark
| 1) Why was this study conducted? |
| To know what non-pharmaceutical interventions (Non-pharmaceutical interventions) have different countries adopted for containment, mitigation, or suppression of COVID-19 pandemic and at what time they were implemented. To review the evidence on the impact of Non-pharmaceutical interventions on containment, mitigation, or suppression of the pandemic. |
| 2) What were the most relevant results of the study? |
| Some countries are mainly focused on establishing travel restrictions, isolation of identified cases, and high-risk people. Others have a more intense combination of drastic social distancing measures like mandatory quarantine measures for the entire population and closure of all educational centers. Some of the countries have implemented drastic social distancing measures in the first fifteen days after detecting the first case, other countries have taken more than 30 days. The effectiveness of isolated Non-pharmaceutical interventions may be limited, but combined interventions have shown to have a high impact in reducing the transmissibility of the disease, the collapse of health care services, and mortality. When the number of new cases has been controlled, it is necessary to maintain social distancing measures. Testing, contact tracing, and quarantine of suspected cases could be the main strategies after the relaxation of drastic social distancing Non-pharmaceutical interventions |
| 3) What do these results contribute? |
| The evidence synthesized might inform the policy decision-making regarding the control of COVID-19 disease. |
Introduction
Coronavirus disease 2019 (COVID-19) is a new, rapidly emerging infectious disease, which constitutes a major global health threat 1 . On January 30th, 2020, the World Health Organization (WHO) declared the outbreak a global health emergency 2 , while Colombia did it on March 12th 3 .
The virus SARS-CoV-2 appears to have high transmissibility, the basic reproduction number (R0) range from 2.8 to 5.5, in the absence of full quarantine and social distancing measures, in comparison to the average R0 for seasonal influenza viruses which is about 1.8 4 .
In past experiences, like the 1918-19 H1N1 influenza pandemic, no effective interventions or vaccines were available to treat or prevent the disease; this has taught us that in these circumstances, a variety of non-pharmaceutical interventions (Non-pharmaceutical interventions) are successful at reducing case numbers 4 . Non-pharmaceutical interventions include isolating ill persons, contact tracing, quarantine of exposed persons, social distancing, travel restrictions, school, churches and workplace closure, and cancellation of mass gathering events 4 - 9 . Those interventions have shown to be effective ways to respond to the outbreak when implemented early in the epidemic (4-6). Past epidemics have also shown that while the interventions remained in place, mortality is reduced; however, “transmission rebounded once controls are lifted” 4 .
Three groups of Non-pharmaceutical interventions strategies have been recognized, 1) containment, 2) mitigation, and 3) suppression 6 , 7 . Containment interventions are those implemented when the first cases are detected in order to interrupt the transmission of the disease, prevent its spread and give time to the healthcare system to make the preparations for attending patients, and waiting for the development of vaccines and effective interventions 9 . Mitigation interventions are used when the number of cases increases and the possibility of finding a relationship between cases is complicated, mitigation is not aimed to interrupt transmission completely, but to reduce the health impact of an epidemic over the mortality and the collapse of the health system 4 , 10 . And suppression is intended to reduce the average number of secondary cases each case generates 4 .
According to the Imperial College, suppression carries enormous social and economic costs, which may themselves have a significant impact on health and well-being in the short and longer-term. Mitigation will never be able to protect those at risk from severe disease or death entirely, and the resulting mortality may, therefore, still be high 4 .
In China, three major Non-pharmaceutical interventions have been implemented to control the spread and reduce the outbreak size of COVID-19 9 . First, inter-city travel bans and the establishment of a cordon sanitaire of Wuhan and surrounding cities in Hubei Province 9 , 11 - 13 . Second, measures for improving the screening, contact tracing, identification, diagnosis, isolation, and reporting of suspected ill persons and confirmed cases 9 , 14 . And third, implementing inner-city travel and contact restrictions, which included limiting individual social contact, using personal hygiene and protective measures, and increasing the physical distance between those who have COVID-19 and those who do not 9 , 15 . The Chinese government also encouraged people to stay at home as much as possible, canceled or postponed large public events and mass gatherings, and closed libraries, museums, and workplaces 8 , 9 .
The progressive spread of the disease has allowed many countries to anticipate that a pandemic is approaching 9 , 16 . In the case of Colombia, some local governments, as well as the national government, rapidly and drastically implemented a quarantine in all the national territory, as well as other Non-pharmaceutical interventions aimed at the contention, suppression, and mitigation of the COVID-19 disease.
The best available scientific evidence is required to design effective Non-pharmaceutical interventions and disseminate the knowledge urgently to help policymakers assess the potential benefits and costs of Non-pharmaceutical interventions to contain COVID-19 outbreaks. It is essential to describe how different countries implement Non-pharmaceutical interventions, and at what point of the epidemic. It is also necessary to explore how those Non-pharmaceutical interventions have impacted the number of cases, the mortality, and the capacity of health care facilities to deliver healthcare services. There are still crucial knowledge gaps on the effectiveness of different interventions to adequately justify the preparation, implementation, or cancellation of various Non-pharmaceutical interventions, policymakers across the World need evidence as to the combination and timings of each, which remains lacking.
Materials and Methods
A rapid evidence synthesis focused on identifying Non-pharmaceutical interventions implemented in the city of Wuhan and 19 countries (i.e., Argentina, Australia, Brazil, Canada, Chile, China, Colombia, Cuba, Germany, Iran, Italy, Japan, Mexico, Norway, Russia, South Korea, Spain, United Kingdom, and the United States) was carried out. Three criteria were applied to select the countries and territories, 1) a comparatively high number of cases, 2) a political or social particularity that allows the understanding of different types of Non-pharmaceutical interventions or different pace in their implementation; and 3) balance between countries in Europe, Asia, and North, Central, and South America.
Eight web pages of transnational organizations, 17 webpages of international magazines and newspapers, and 99 webpages of governmental institutions in the 19 countries included were searched from January 1st to March 25th, 2020. Additionally, the databases Medline and Embase were searched for studies evaluating the effectiveness of Non-pharmaceutical interventions for the containment, suppression, and mitigation of COVID-19 (Appendix 1with the search sources).
Official documents and media articles were used to determine the date when different countries implemented Non-pharmaceutical interventions. The eligibility criteria of academic papers were that the article was focused on exploring the effectiveness and impact of Non-pharmaceutical interventions on the containment, suppression, or mitigation of COVID-19, with no language, neither study design restrictions. Eligible studies included observational studies (cohorts, time series, series report), simulations studies, and health system or political system guidance.
Quality assessment of observational studies was performed with the Johana Briggs criteria for appraisal. In contrast, simulation studies were not formally quality assessed. Still, a judgement was provided according to the completeness of variables to perform the simulation, the strength of the assumptions, and the quality of the description of the statistical procedure. All stages of the review process were performed by one researcher and checked by a second.
Information about the number of new cases and new deaths caused by COVID-19 in the countries and territories chosen was reached from the John Hopkins Center for Systems Science and Engineering after realizing that its dashboard has more updated information than the situation reports of WHO 1 . The first case reported in each country was documented from official sources or from WHO, with this information, we determined how many days elapsed between the first case reported and the NPI decision taken by the government. The number of days to make the decision was used to develop a timeline of events, a heat map, and a joint figure that represents new cases day by day and the point in which the Non-pharmaceutical interventions were decided. The heat map was developed with R software 17 .
Results
All countries have implemented several Non-pharmaceutical interventions to control COVID-19 infection. However, there is variability in the amount and type of interventions. In countries like Brazil, Canada, Mexico, and Russia, we identified few interventions, and none of them were among the most drastic measures of social distancing, for example, Mexico has only implemented the closure of schools and colleges 18 . These countries have focused mainly on avoiding the entry of cases by using travel restrictions and isolating the identified cases and high-risk people.
Another group of countries applied several interventions, including one of the drastic social distancing ones. South Korea, United Kingdom, and the United States, for example, have implemented more drastic social distancing interventions combined with rules of detection, contact tracing, and isolation of cases and contacts. Notably, South Korean is recognized for the rapid implementation of a mass case detection strategy 19 , while recently in some of the States in the United States have begun the implementation of social distancing measures 20 .
The third group of countries has applied an intense combination of drastic interventions for containment, mitigation, and suppression of infection. Argentina, Chile, China, Colombia, Italy, Spain, all implemented mandatory quarantine for the entire population, after closing schools and universities, canceling all events that concentrated more than 200 people and suspending public transportation for all who do not carry out essential work for infection control. In addition, they have also employed case isolation and contact tracing, borders closings, and some are implementing mass case detection.
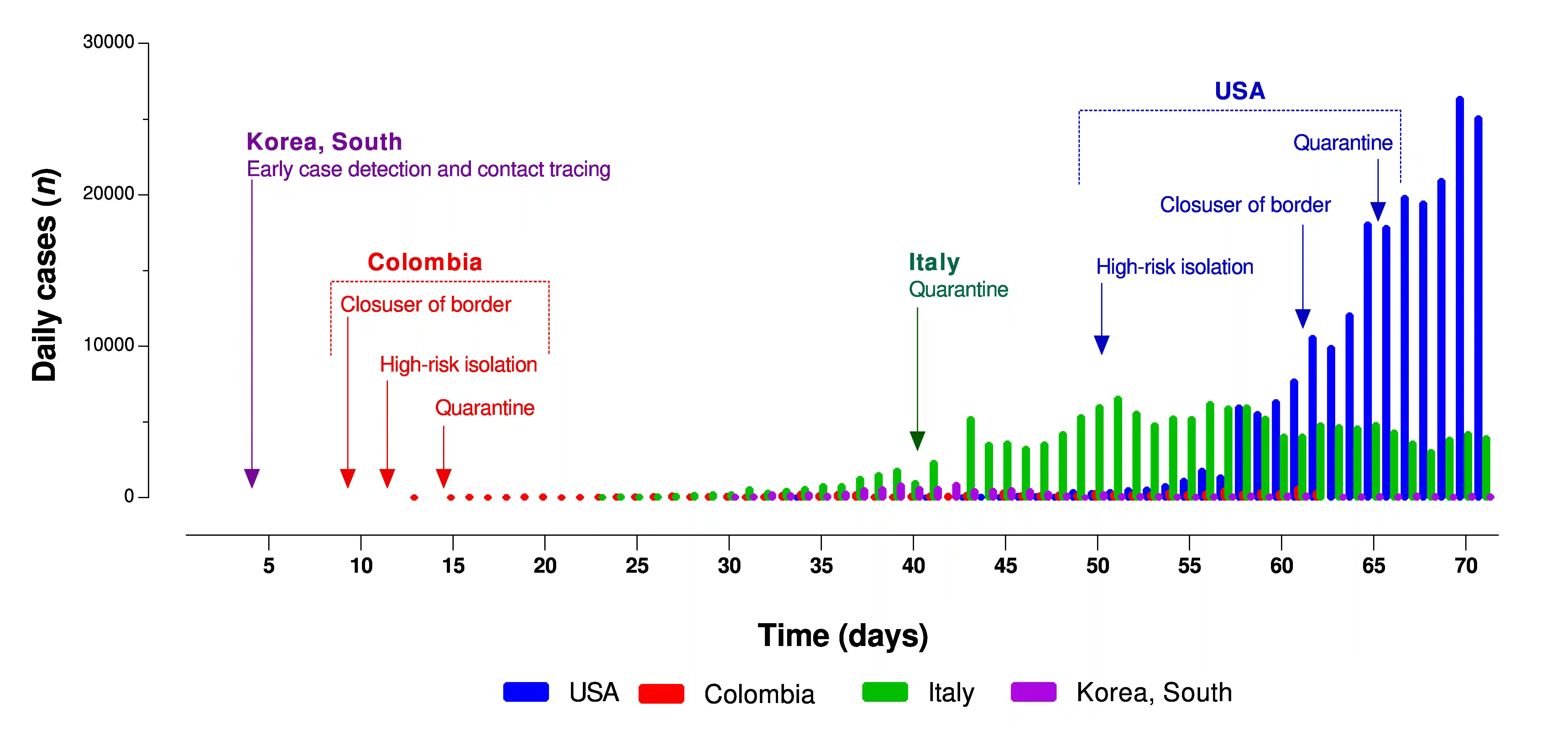
Regarding the pace for implementing the strategies, some countries such as Argentina, Chile, and Colombia, which reported the first case in March, implemented interventions in the early fifteen days after the detection of the first case (Table 1 for further details), or even before the notification of the first case, as it is the case of Chile. Argentina, Chile, and Colombia have had the opportunity to anticipate and learn from the policy decision made in other countries, such as China and South Korea, affected as early as December 2019 and January 2020 (Figure 1 that exhibits a heat map of the time to implement the interventions). Countries such as Italy, Spain, and the United States, took more than 30 days to implement drastic measures of social distancing, and they are displaying an extreme situation of the collapse of their health systems. These experiences have served to apprentice countries to making decisions early after the first case is reported (Figure 2 for information about the moment in which some countries have implemented some decisions and the number of new cases they had at that time).
Table 1. Non-pharmaceutical interventions and number of days to implement them after the first case of COVID-19 (as march 28 of 2020).
| Countries/first case date | Hubei | China | Japan | Korea | United States | Australia | Canada | Germany | Spain | Italia | Russia | United Kingdom | Iran | Brazil | Norway | México | Chile | Argentina | Colombia | Cuba |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 31/12/19 | 31/12/2019 | 15/01/20 | 20/01/20 | 21/01/20 | 26/01/20 | 27/01/20 | 27/01/20 | 31/01/20 | 31/01/20 | 1/02/20 | 1/02/20 | 20/02/20 | 26/02/20 | 27/02/20 | 29/02/20 | 3/03/20 | 3/03/20 | 6/03/20 | 13/03/20 | |
| Measures | ||||||||||||||||||||
| Emergency declaration | 23 | 13 | 52 | 53 | 43 | 9 | 25 | -24 | 9 | 6 | ||||||||||
| Population level social distancing | ||||||||||||||||||||
| Quarantine | 23 | 24 | 62* | 59 | 38 | 52 | 18 | 16 | 16 | |||||||||||
| Closing schools and universities | 23 | 48 | 43 | 41 | 30 | 5 | 14 | 14 | 12 | 12 | 10 | 11 | ||||||||
| Canceling of large events | 20 | 54 | 43 | 39 | 39 | 14 | 15 | 14 | 6 | |||||||||||
| Suspension of public transportation | 23 | 41 | 51 | 35 | 14 | |||||||||||||||
| Isolation of cases and contacts | ||||||||||||||||||||
| Isolation of travelers from china | 20 | 50 | 2 | 34 | -18 | -41 | -26 | 4 | ||||||||||||
| Isolation of travelers from other countries | 62 | 49 | 58 | 33 | 34 | 15 | 3 | 3 | 4 | 7 | ||||||||||
| Isolation of high-risk population | 46 | 34 | 53 | 38 | 49 | 18 | 16 | 19 | 14 | 12 | -45 | |||||||||
| Isolation of cases or symptomatic people | 31 | 46 | 40 | 14 | 18 | -41 | 8 | |||||||||||||
| Travel restrictions | ||||||||||||||||||||
| Entry restrictions for foreigners (China) | 19 | 2 | 10 | 54 | 49 | 30 | -1 | 14 | -46 | 14 | 9 | 9 | ||||||||
| Entry restrictions for foreigners (Others) | 61 | 59 | 39 | 54 | 49 | 43 | 39 | 27 | 22 | 16 | 15 | 14 | 12 | 9 | ||||||
| Closure of borders | 57 | 54 | 51 | 51 | 44 | 26 | 14 | 15 | 13 | 10 | 7 | |||||||||
| International travel restrictions | 54 | 58 | 58 | 54 | 48 | 39 | 38 | 32 | 46 | 25 | 16 | 15 | 9 | |||||||
| Inter-city travel restrictions | 31 | 31 | 54 | 48 | 38 | 41 | 25 | 17 | 14 | 16 | ||||||||||
| Early case detection and contact tracing | ||||||||||||||||||||
| Intensive early case detection | 20 | 21 | 6 | 6 | 19 | 44 | 5 | 8 | -32 | 5 | ||||||||||
| Contac tracing | 20 | 21 | 33 | 6 | 10 | -41 | 10 | |||||||||||||
Figure 1. Heat map of Non-pharmaceutical interventions and number of days in which they were implement them after the first case of COVID-19.
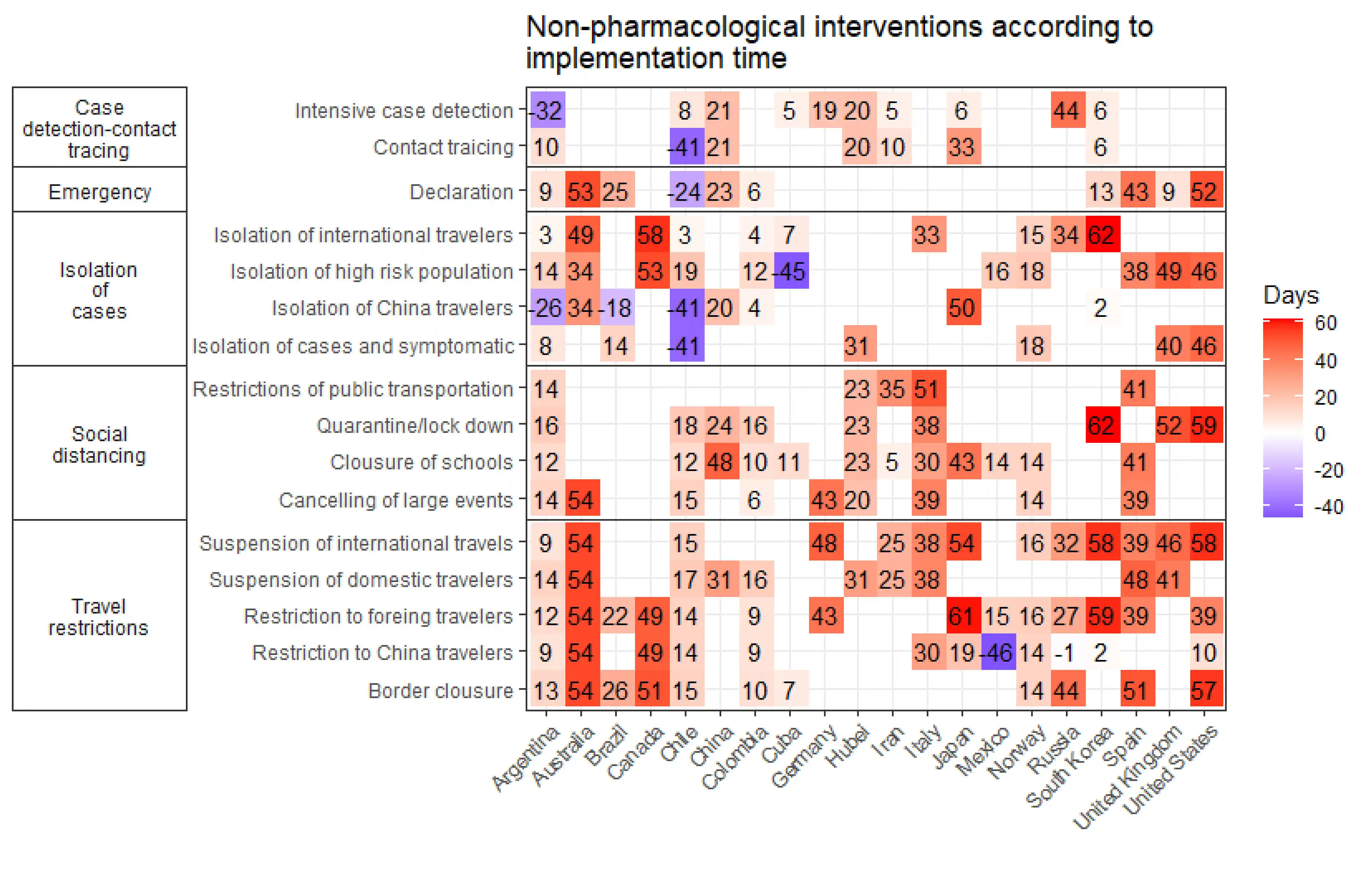
Figure 2. Number of new COVID-19 cases and day of implementation of some Non-pharmaceutical interventions .
Other Non-pharmaceutical interventions implemented by the countries analyzed include interventions to improve the infrastructure of the health system and strength the human resources capacity (e.g., expand the capacity of beds, enable the use of stadiums and other spaces), strategies aimed at populations at risk (e.g., special measures for the people deprived of liberty), social support interventions (e.g., tax relieves), strategies to support the production of goods and services (e.g., facilitate loans to companies), and strategies for accurate information, timely communication, and support for social distancing (Appendix 2).
Impact of Non-pharmaceutical interventions
In exploring the effectiveness of non-pharmaceutical interventions on containment, suppression, and mitigation of COVID-19 infection, we included nine over 34 studies identified (one policy guidance, one rapid systematic review, two cohort studies, one time series study, and four simulations) 4 - 6 , 11 - 13 , 21 , 22 . Appendix 3 summarizes the findings of these studies.
The effectiveness of any isolated Non-pharmaceutical interventions may be limited, but combined interventions have shown to be effective and have a high impact in reducing the transmissibility of the disease, the collapse of health care services, and mortality. Seven of nine studies included explicitly suggest the early implementation of combined and strict interventions; mainly, quarantine, social distancing, suspension of public transportation, early detection of cases and home isolation of mild cases 4 , 5 , 9 , 12 , 13 , 21 , 22 (Table 2).
Table 2. Impact of non-pharmaceutical interventions for the control of COVID-19 infection.
| No-Pharmaceutical Intervention | Impact | # of studies addressing the intervention | Type of study |
|---|---|---|---|
| Combination of interventions | High | 7 | 1 policy guidance |
| 2 cohort studies | |||
| 1 rapid systematic review | |||
| 1 time series study | |||
| 2 simulations | |||
| Isolation of cases | High | 3 | 1 policy guidance |
| 2 simulations | |||
| Early detection of cases | High | 2 | 1 policy guidance |
| 1 simulation | |||
| Contact tracing | High | 1 | 1 simulation |
| Quarantine of contacts | High | 2 | 1 cohort study |
| 1 policy guidance | |||
| Suspension of public transportation | High | 2 | 1 rapid systematic review |
| 1 cohort study | |||
| Canceling of large events | High | 2 | 1 rapid systematic review |
| 1 cross-sectional study | |||
| Maintaining social distancing interventions for at least 6 months after the outbreak | High | 2 | 2 simulations |
| Self-isolation of symptomatic people | Moderately high | 2 | 1 policy guidance |
| 1 simulation | |||
| Isolation of people older than 70 years | Moderate | 1 | 1 simulation |
| Work at home strategies | Moderate | 1 | 1 policy guidance |
| Social distancing | Moderately low | 3 | 2 simulations |
| 1 rapid systematic review | |||
| Inner-city travel restrictions | Moderately low | 2 | 1 policy guidance |
| 1 simulation | |||
| Inter-city travel restrictions | Moderately low | 3 | 1 policy guidance |
| 1 cohort study | |||
| 1 cross-sectional study | |||
| Closure of schools and daycares | Moderately low | 2 | 1 policy guidance |
| 1 simulation | |||
| Quarantine of people traveling from territories affected | Low | 1 | 1 cohort study |
| Contact reduction | Low | 1 | 1 simulation |
| Closure of borders | Low | 1 | 1 policy guidance |
| Procedures for detecting cases in the airports | Low | 1 | 1 policy guidance |
Without the implementation of Non-pharmaceutical interventions, one study in China claims that the number of COVID-19 cases would have a 51-fold increase in Wuhan, a 92-fold increase in other Hubei cities, and a 125-fold increase in other provinces 9 . Combined Non-pharmaceutical interventions might reduce the maximum demand for medical care and mortality by half or even two thirds 4 . A simulation study for the United Kingdom and the United States shows that, in an uncontrolled epidemic, demand for intensive care beds is predicted to exceed as early as the second week of April, with peak demand for care beds of more than 30 times the maximum supply in both countries 4 .
After the peak of the disease, and when the number of new cases has been controlled, it is necessary to maintain social distancing measures, control of public transportation, work-at-home strategies, case detection and isolation, and contact tracing. Contact tracing and case isolation are suggested to be highly effective in controlling a new COVID-19 outbreak. However, the probability of control decreases with 1) long delays from onset of symptoms until deciding isolation, 2) few contacts tracked per case, and 3) when the transmission before symptoms increases 22 . In most of the simulation scenarios and from the public health experience of previous epidemics, it is identified that, if the social contact resumes to normal levels, the contagions could increase again. Therefore several Non-pharmaceutical interventions, including social distancing, should be continued for several months, 9 it is even proposed that restrictive measures should be maintained until a vaccine is available (potentially 18 months or more) since it is predicted that transmission will recover quickly if interventions are relaxed 4 .
When the number of new cases demonstrates the control of the disease, evidence suggests that measures that can be lifted first are border closures, case detection procedures at airports, and the closings of schools and daycares. The evidence also suggests that both the establishment and removal of Non-pharmaceutical interventions depend on several political, social, and cultural factors, not only on the behavior of the disease 5 , 9 , 21 .
Discussion
Summary of the main findings
We consulted eight web pages of transnational organizations, 17 of international media, 99 of government institutions in the 19 countries included, and besides, we included nine studies (out of 34 identified) that met inclusion criteria. We found that some countries are mainly focused on establishing travel restrictions, isolation of identified cases, and high-risk people. Others have a more intense combination of mandatory quarantine for the entire population, closure of all educational centers, and suspension of public transportation for all those who do not perform essential work. Some of the countries have implemented interventions in the first fifteen days after detecting the first case, while others have taken more than 30 days to implement drastic measures of social distancing. The effectiveness of isolated Non-pharmaceutical interventions may be limited, but combined interventions have shown to be effective and have a high impact in reducing the transmissibility of the disease, the collapse of health care services, and mortality. When the number of new cases has been controlled, it is necessary to maintain social distancing measures, public transportation control, work at home strategies, case detection, self-isolation, and contact tracing for several months.
Comparison with other studies
A modeling study made in Colombia to predict the impact of the COVID-19 pandemic according to mitigation measures that have been implemented in the country resonates with our findings that combined interventions could be effective and have a high impact on reducing the transmissibility of the disease. The study of González-Jaramillo et al. 23 , concludes that the combination of mitigation strategies taken by the Colombian government could reduce the number of patients that would require intensive care units from 36,782 in the scenario of no intervention to 1,176 in the scenario that combines case isolation, home quarantine, and social distancing of people over 70 years old.
Our finding of the need to maintain social distancing measures, control of public transportation, work-at-home strategies, case detection and isolation, and contact tracing has also been supported in the literature. The model developed by Prem et al., suggests that the sudden lifting of interventions could lead to an earlier secondary peak, which could be prevented by relaxing the interventions gradually 14 . In this regard, Colburn suggests that testing, contact tracing, and quarantine of suspected cases could be the main strategies after the relaxation of drastic social distancing Non-pharmaceutical interventions to prevent healthcare system overload. Colburn calls for the incorporation of these strategies into models to allow countries to have a better picture of the testing capacity they will need and to decide if such policies could be successful in suppressing COVID-19 spread in a given country 24 .
Non-pharmaceutical interventions also have adverse effects on individuals, communities, and the national economy. A recent rapid review reported that quarantine could have harmful psychological effects such as post-traumatic stress symptoms, confusion, and anger, which can lead to adverse long-term psychological effects 21 , 25 . Many articles have highlighted the economic implications that quarantine interventions might have over the economy in 2020; however, the goal at this moment is saving as many lives as our resources allowed 4 , 5 , 8 , 9 , 12 , 13 , 21 , 26 .
Limitations of this review
Given the time constraints imposed by the ongoing coronavirus outbreak, we made some critical methodological decisions that need to be considered. The inclusion criteria and the extraction of information of the studies included in this synthesis were applied by one reviewer. In addition, simulation studies were not formally quality assessed.
Conclusion
The policy decision-making in this time should be aimed to optimize the opportunities of saving lives, reducing the collapse of health services, and minimizing the economic and social impact over the general population, but principally over the most vulnerable. The timing of implementing and lifting interventions is likely to have a substantial effect on those objectives.
Acknowledgements
The authors want to thank Ivan Dario Flórez and Gabriel Jaime Otálvaro for their important comments and suggestions. They also thank Cristian David Santa Escobar for his contribution in the graphic representation of the results.
Appendix 1. Search sources.
WHO PAHO. WHO Situation Dashboard. https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
WHO. 2019 Novel Coronavirus (2019nCoV): Strategic preparedness and response plan. 03 de Febrero. https://www.who.int/docs/default-source/coronaviruse/srp-04022020.pdf
Enfermedad por el Coronavirus (COVID-19). https://www.paho.org/es/temas/coronavirus/enfermedad-por-coronavirus-covid-19
UNION EUROPEA
Eurosurvelliance. https://www.eurosurveillance.org/content/eurosurveillance/browse
EU Commision COVID-19 Coronavirus data. https://data.europa.eu/euodp/en/data/dataset/covid-19-coronavirus-data/resource/62eb477f-be00-462a-831a-594095f7306a
Politico. Coronavirus in Europe https://www.politico.eu/coronavirus-in-europe/
ECDC. European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en
IATA. International Air Transport Association. Government Measures Related to Coronavirus (COVID-19). https://www.iata.org/en/programs/safety/health/diseases/government-measures-related-to-coronavirus/
Johns Hopkins University and Medicine. Coronavirus Resource Center. Interactive maps and news https://coronavirus.jhu.edu/
COVID-19 Expert Reality Check. Johns Hopkins Bloomberg School of Public Health. https://www.globalhealthnow.org/2020-02/coronavirus-expert-reality-check#quammen
Worldometer owned by Dadax. https://www.worldometers.info/coronavirus/
Evidence Aid https://www.evidenceaid.org/coronavirus-resources/
Otros medios de comunicación
Science Magazine. Mass testing, school closings, lockdowns: Countries pick tactics in ‘war’ against coronavirus. By Jon Cohen, Kai KupferschmidtMar. 18, 2020 , 11:30 AM. https://www.sciencemag.org/news/2020/03/mass-testing-school-closings-lockdowns-countries-pick-tactics-war-against-coronavirus
The Economist. The politics of pandemics. All governments will struggle. Some will struggle more than others. https://www.economist.com/leaders/2020/03/12/the-politics-of-pandemics
Prospect Magazine UK. Coronavirus: Why scientists are divided over the effectiveness of the UK’s strategy by Philip Ball / March 16, 2020. https://www.prospectmagazine.co.uk/science-and-technology/coronavirus-uk-herd-immunity-boris-johnson-government-plan-cure
StateNews. Understanding what works: How some countries are beating back the coronavirus by Helen Branswell March 20, 2020. https://www.statnews.com/2020/03/20/understanding-what-works-how-some-countries-are-beating-back-the-coronavirus/
The NY Times. The Coronavirus Outbreake https://www.nytimes.com/news-event/coronavirus?action=click&pgtype=Article&state=default&module=STYLN_coronahub&variant=show®ion=header&context=menu
Wikipedia . Resumen de decisiones de los gobiernos. https://en.wikipedia.org/wiki/National_responses_to_the_2019%E2%80%9320_coronavirus_pandemic
International restrictions. https://en.wikipedia.org/wiki/Travel_restrictions_related_to_the_2019%E2%80%9320_coronavirus_pandemic
BBC News. Coronavirus pandemic. https://www.bbc.com/news/explainers
The Guardian. Coronavirus Outbreak. https://www.theguardian.com/world/coronavirus-outbreak
The Washington Post. Coronavirus news and maps. https://www.washingtonpost.com/world/2020/03/27/coronavirus-latest-news/
Aljazeera. Coronavirus Pandemic News. https://www.aljazeera.com/topics/events/coronavirus-outbreak.html
El Espectador. Coronavirus hoy: ¿Qué están haciendo otros países de América Latina para contener la pandemia?. https://www.elespectador.com/noticias/el-mundo/coronavirus-hoy-que-estan-haciendo-otros-paises-de-america-latina-para-contener-la-pandemia-articulo-910367
¿Qué está haciendo cada país de América Latina para frenar el nuevo coronavirus?. https://rpp.pe/mundo/actualidad/coronavirus-covid-19-que-esta-haciendo-cada-pais-de-america-latina-para-frenar-el-nuevo-coronavirus-noticia-1252868
Semana. Semana Tendencias Coronavirus. https://www.semana.com/noticias/coronavirus/126948
El Colombiano. Coronavirus en Colombia contra el miedo. https://www.elcolombiano.com/coronavirus-en-colombia-contra-el-miedo
Europapres. Agencia Europa Press https://www.europapress.es/
RFI. Noticias Coronavirus http://www.rfi.fr/es/tag/coronavirus/
CNN Noticias Coronavirus CNN https://cnnespanol.cnn.com/category/coronavirus.
Note: The following official sources and other media were consulted between March 16 and March 27 to identify the actions and strategies defined by the countries.
ALEMANIA
Fuentes Oficiales
Federal Ministry of Health. https://www.bundesgesundheitsministerium.de/en/press/2020/coronavirus.html#c17182
Robert Koch Institute. https://www.rki.de/EN/Home/homepage_node.html
The Federal Government. Together against Corona. https://www.zusammengegencorona.de/
Chancellor and Federal Government. https://www.bundesregierung.de/breg-en/search/998964!search
Otros medios de comunicación
Deutsche Welle. Coronavirus. https://www.dw.com/en/top-stories/coronavirus/s-32798
Coronavirus en Alemania: últimas noticias. https://www.deutschland.de/es/news/coronavirus-en-alemania-actualizaciones
Noticias Bundesliga. https://www.bundesliga.com/es/bundesliga/noticias/noticias-informacion-actualidad-liga-alemana-3034-2316
Pressemitteilungen. https://www.bundesgesundheitsministerium.de/presse/pressemitteilungen/2020/1-quartal/krisenstab-bmg-bmi-sitzung-5.html
Bundesministeriums für Verkehr und digitale Infrastruktur. https://www.bmvi.de/DE/Ministerium/Minister-Staatssekretaere/minister-staatssektretaere.html
Coronavirus: Jens Spahn trifft Gesundheitsminister der Länder. https://www.youtube.com/watch?v=nm5l-uxSeeM&feature=youtu.be
Statement von Jens Spahn bei Pressekonferenz vom 19.03.2020. https://www.youtube.com/watch?v=9dQKFImYaY0&feature=youtu.be
ARGENTINA
Fuentes Oficiales
Ministerio de Salud. Coronavirus. https://www.argentina.gob.ar/salud/coronavirus-COVID-19
Gobierno Nacional. Resumen de medidas. https://www.argentina.gob.ar/coronavirus/medidas-gobierno
Otros medios de comunicación
El Clarin. Coronavirus en Argentina: piden donaciones para ayudar a los que menos tienen. https://www.clarin.com/sociedad/coronavirus-argentina-piden-donaciones-ayudar_0_9O4v1s5nJ.html
Infoabae. Argentina solo recibió ayuda de China para enfrentar la pandemia del coronavirus. https://www.infobae.com/politica/2020/03/22/la-argentina-solo-recibio-ayuda-sanitaria-de-china-para-enfrentar-la-pandemia-del-coronavirus/
RSE Presente. En épocas de coronavirus una ONG contagia solidaridad. https://presenterse.com/en-epocas-de-coronavirus-una-ong-que-contagia-solidaridad/
AUSTRALIA
Fuentes Oficiales
Coronavirus: COVID-19: Western Australian Government response. https://www.wa.gov.au/organisation/department-of-the-premier-and-cabinet/coronavirus-covid-19-western-australian-government-response
Safe Work Australia. https://www.safeworkaustralia.gov.au/doc/coronavirus-covid-19-advice-employers
COVID-19 (Coronavirus) and the Australian border. https://www.homeaffairs.gov.au/news-media/current-alerts/novel-coronavirus
COVID-19 Coronavirus Information for Public Sector Employers. https://www.commerce.wa.gov.au/labour-relations/covid-19-coronavirus-information-public-sector-employers
Departamento de salud Gobierno de Australia. https://www.health.gov.au/news
Health information for western Australia. https://www.healthywa.wa.gov.au/Articles/A_E/COVID-clinics
Conferencia de prensa primer ministro de Australia. https://www.pm.gov.au/media/transcript-press-conference
Actualización medidas primer ministro. https://www.pm.gov.au/media/update-coronavirus-measures
Circular 5/2020 - Licencia COVID-19 y otras flexibilidades laborales. https://www.commerce.wa.gov.au/sites/default/files/atoms/files/pslr_circular_04_2020.pdf
BRASIL
Fuentes Oficiales
Agencia Nacional de Vigilancia Sanitaria. http://portal.anvisa.gov.br/
Ministerio de salud. https://www.saude.gov.br/noticias
Otros medios de comunicación
Infoabae. Brasil cerró sus fronteras a europeos y asiáticos por el coronavirus. https://www.infobae.com/america/america-latina/2020/03/20/brasil-cerro-sus-fronteras-a-europeos-y-asiaticos-por-el-coronavirus/
CANADÁ
Fuentes Oficiales
Public Health Agency of Canada. https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19.html
Página oficial Primer ministro. https://pm.gc.ca/
Página oficial- Gobierno de Canadá. https://www.canada.ca/
CHINA Y HUBEI
Fuentes Oficiales
Chinese Center for Disease Control and Prevention. http://www.chinacdc.cn/en/COVID19/
National Health Commission of the People's Republic of China. http://en.nhc.gov.cn/antivirusfight.html
CHILE
Fuentes Oficiales
Plan de Acción Coronavirus. https://www.gob.cl/coronavirus/
Ministerio de Salud. Seguimiento de casos. https://www.minsal.cl/nuevo-coronavirus-2019-ncov/casos-confirmados-en-chile-covid-19/
Ministerio de Relaciones Internacionales. Medidas. https://chile.gob.cl/chile/medidas-de-prevencion-ante-el-nuevo-coronavirus
Servicio Informativo del Instituto de Previsión Social. Ministerio del Trabajo. https://www.chileatiende.gob.cl/coronavirus
Fuentes Oficiales
Ministerio de Salud y Protección Social. Coronavirus. https://d2jsqrio60m94k.cloudfront.net/
Ministerio de salud. https://www.minsalud.gov.co/
Instituto Nacional de Salud. https://www.ins.gov.co/Noticias/Paginas/Coronavirus.aspx
Presidencia de la República. https://id.presidencia.gov.co
Ministerio de Transporte. https://www.mintransporte.gov.co
Aeronáutica Civil de Colombia. http://www.aerocivil.gov.co/
COREA DEL SUR
Korean Centers for Disease Control and Prevention. http://www.cdc.go.kr/board.es?mid=a30402000000&bid=0030
CUBA
Fuentes Oficiales
Presidencia de Cuba. Noticias y medidas. https://www.presidencia.gob.cu/es/noticias/
Ministerio de Comercio. Medidas coronavirus. https://www.mincin.gob.cu/content/medidas-de-protecci%C3%B3n-tomadas-en-el-sector-del-comercio-para-prevenir-cualquier-contagio-0
Ministerio Relaciones Internacionales. Medidas coronavirus. http://misiones.minrex.gob.cu/es/coronavirus
Ministerio de Salud Pública de la República de Cuba. https://salud.msp.gob.cu/
Otros medios de comunicación
Cibercuba. Mapa del Coronavirus en Cuba. https://www.cibercuba.com/tags/coronavirus-cuba
Infomed, Portal de la Red de Salud de Cuba. http://www.sld.cu/
ESPAÑA
Fuentes Oficiales
Alertas en Salud Pública de actualidad. MinSalud España. https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/home.htm
Instituto de Salud Carlos III. Situación de COVID-19 en España. https://covid19.isciii.es/
Portal de La Moncloa. https://www.lamoncloa.gob.es/Paginas/buscadoravanzado.aspx
Instituto de Mayores y Servicios Sociales. https://www.imserso.es/imserso_02/actualidad/2020/marzo/IM_130154
Ministerio del Interior no a Penitenciarias. www.interior.gob.es
Otros medios de comunicación
Lista de Medidas del gobierno de El Diario. https://www.eldiario.es
ESTADOS UNIDOS
Fuentes Oficiales
Centers for Disease Control and Prevention. https://www.cdc.gov/
Página oficial del coronavirus de CDC. https://www.coronavirus.gov
White house. https://www.whitehouse.gov/
Departamento de Estado. https://travel.state.gov/
Departamento de defensa. https://www.defense.gov/
Asociación de médicos de los Estados Unidos. https://www.ama-assn.org
Gobierno de los Estados Unidos. https://www.usa.gov/
ITALIA
Fuentes Oficiales
Ministero della Salute. Nuovo coronavirus. http://www.salute.gov.it/nuovocoronavirus
Ministero della Salute. Situazione in Italia. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5351&area=nuovoCoronavirus&menu=vuoto
Protezione Civile. Emergenza Coronavirus. http://www.protezionecivile.gov.it/
Instituto Superiore di Sanitá. http://www.iss.it/coronavirus
Trova norme salute. http://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73532
Guida per prevenire e affrontare lo stigma sociale. http://www.salute.gov.it/imgs/C_17_notizie_4149_0_file.pdf
Aeroporti di Roma. http://www.adr.it/it/web/guest/coronavirus
Governo Italiano Presidenza del Consiglio dei Ministri. http://www.governo.it/it/articolo/comunicato-stampa-del-consiglio-dei-ministri-n-33/14204
L'epidemiologia per la sanità pubblica Istituto Superiore di Sanità. https://www.epicentro.iss.it/
IRÁN
Fuentes Oficiales
Ministry of Health and Medical Education. News. http://irangov.ir/cat/509
Ayatollah Khamenei. Official website. http://english.khamenei.ir/
Otros medios de comunicación
Islamic Republic News Agency. https://en.irna.ir/ y https://es.irna.ir/
Iran Daily. http://www.iran-daily.com/
JAPÓN
Fuentes Oficiales
Ministry of Health, Labour and Welfare. About coronavirus Disease 2019. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html
Prime Minister of Japan and His Cabinet. Basic responses to COVID2019. http://japan.kantei.go.jp/ongoingtopics/coronavirus_info_e.html
MÉXICO
Fuentes Oficiales
Gobierno de México. Comunicados y decisiones. https://coronavirus.gob.mx/noticias/
Dirección General de Epidemiología. Mapa de casos. http://ncov.sinave.gob.mx/mapa.aspx
Sistema de Información de la Secretaría de Salud. http://sinaiscap.salud.gob.mx:8080/DGIS/
Instituto Mexicano del Seguro Social. http://www.imss.gob.mx/
Otros medios de comunicación
Diario AS México. Covid-19. https://mexico.as.com/tikitakas/tag/covid_19/a/
NORUEGA
Fuentes Oficiales
Norwegian Institute of Public Health. https://www.fhi.no/en/id/infectious-diseases/coronavirus/
Ministry of Health and Care Services. https://www.regjeringen.no/en/dep/hod/id421/
REINO UNIDO
Fuentes Oficiales
Government UK. Coronavirus. https://www.gov.uk/coronavirus
Coronavirus (COVID-19): UK government response. https://www.gov.uk/government/topical-events/coronavirus-covid-19-uk-government-response
The Health Protection (Coronavirus) Regulations 2020. http://www.legislation.gov.uk/uksi/2020/129/contents/made
Public Health England. https://www.gov.uk/government/organisations/public-health-england
Departamento de salud pública Inglaterra. https://www.gov.uk/government/organisations/department-of-health-and-social-care
Oficina del primer ministro. https://www.gov.uk/government/organisations/prime-ministers-office-10-downing-street
Ministerio de comunidades y gobierno local. https://www.gov.uk/government/organisations/ministry-of-housing-communities-and-local-government
Departamento de trabajo y pensiones. https://www.gov.uk/government/organisations/department-for-work-pensions
Departamento de negocios, energía e industria. https://www.gov.uk/government/organisations/department-for-business-energy-and-industrial-strategy
http://www.legislation.gov.uk/ukpga/1984/22
Foreign Travel Advice. https://www.gov.uk/foreign-travel-advice
Foreign & Commonwealth Office. https://www.gov.uk/government/organisations/foreign-commonwealth-office
Noticias gobierno de UK. https://www.gov.uk/government/news/
Statutory Sick Pay. Pago estatutario de enfermedad. https://www.gov.uk/statutory-sick-pay
Portal de noticias NHS. https://www.england.nhs.uk/2020/03/nhs-111-online-to-help-people-with-coronavirus/
Appendix 2.
Appendix 2. Non-pharmaceutical interventions and number of days in which they were implemented (as March 28, 2020).
| Country/First case date | Hubei | China | Japan | South Korea | United States | Australia | Canada | Germany | Spain | Itally | Russia | United Kingdom | Iran | Brazil | Norway | Mexico | Chile | Argentina | Colombia | Cuba |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 31/12/2019 | 31/12/2019 | 15/01/2020 | 20/01/2020 | 21/01/2020 | 26/01/2020 | 27/01/2020 | 27/01/2020 | 31/01/2020 | 31/01/2020 | 1/02/2020 | 1/02/2020 | 20/02/2020 | 26/02/2020 | 27/02/2020 | 29/02/2020 | 3/03/2020 | 3/03/2020 | 6/03/2020 | 13/03/2020 | |
| Strategies | ||||||||||||||||||||
| Declaration of emergency | 23 | 13 | 52 | 53 | 43 | 9 | 25 | -24 | 9 | 6 | ||||||||||
| Social distancing at population level | ||||||||||||||||||||
| Mandatory quarantine throughout the territory (or part of it) | 23 | 24 | 62 | 59 | 38 | 52 | 18 | 16 | 16 | |||||||||||
| Suspension of face-to-face classes in kindergartens, schools or universities | 23 | 48 | 43 | 41 | 30 | 5 | 14 | 14 | 12 | 12 | 10 | 11 | ||||||||
| Closure of cinemas, restaurants, and other social-meeting places | 23 | 55 | 37 | 48 | 14 | 17 | 14 | 12 | ||||||||||||
| Closure of public parks (museums included) | 20 | 41 | 49 | 5 | 14 | 14 | 12 | |||||||||||||
| Suspension of gatherings | 20 | 54 | 43 | 39 | 39 | 14 | 15 | 14 | 6 | |||||||||||
| Suspension of non-essential activities | 14 | 14 | ||||||||||||||||||
| Prohibition of mobility in public or private means of transport | 23 | 41 | 51 | 35 | 14 | |||||||||||||||
| Social distancing of cases or contacts | ||||||||||||||||||||
| Isolation for 14 days because of attending places with high influx of people | 4 | |||||||||||||||||||
| Isolation because of coming from China | 20 | 50 | 2 | 34 | -18 | -41 | -26 | 4 | ||||||||||||
| Isolation because of coming from another country | 62 | 49 | 58 | 33 | 34 | 15 | 3 | 3 | 4 | 7 | ||||||||||
| Isolation because of living with a possible positive case | 14 | -41 | 14 | |||||||||||||||||
| Isolation because of being a person at high risk of contracting the virus | 46 | 34 | 53 | 38 | 49 | 18 | 16 | 19 | 14 | 12 | -45 | |||||||||
| Isolation because of presenting symptoms or being a positive case | 31 | 46 | 40 | 14 | 18 | -41 | 8 | |||||||||||||
| Travel restrictions | ||||||||||||||||||||
| Entry restrictions for foreigners (China) | 19 | 2 | 10 | 54 | 49 | 30 | -1 | 14 | -46 | 14 | 9 | 9 | ||||||||
| Entry restrictions for foreigners (other countries) | 61 | 59 | 39 | 54 | 49 | 43 | 39 | 27 | 22 | 16 | 15 | 14 | 12 | 9 | ||||||
| Border closure for non-essential Traffic | 57 | 54 | 51 | 51 | 44 | 26 | 14 | 15 | 13 | 10 | 7 | |||||||||
| Restrictions on international travels | 54 | 58 | 58 | 54 | 48 | 39 | 38 | 32 | 46 | 25 | 16 | 15 | 9 | |||||||
| Restrictions on domestic air travel | 31 | 31 | 54 | 48 | 38 | 41 | 25 | 17 | 14 | 16 | ||||||||||
| Restrictions on cruise ships | 36 | 54 | 41 | 40 | 12 | 12 | 6 | |||||||||||||
| Case tracking and detection | ||||||||||||||||||||
| Intensive case search (in port of entry and in all territorial entities/provinces) | 20 | 21 | 6 | 6 | 19 | 44 | 5 | 8 | -32 | 5 | ||||||||||
| Contact tracking | 20 | 21 | 33 | 6 | 10 | -41 | 10 | |||||||||||||
| Use of technology to detect cases, track contacts, and notify (e.g., thermometers, drive-through, apps) | 14 | 14 | 6 | 43 | 47 | 34 | -41 | 15 | ||||||||||||
| Labs or additional capabilities | 27 | 34 | 21 | 56 | 44 | 44 | 6 | 5 | 18 | -4 | 15 | |||||||||
| Infrastructure of the health and human resource system | ||||||||||||||||||||
| Expanding the capacity of beds | 34 | 34 | 46 | 41 | 19 | -1 | 4 | 15 | 6 | |||||||||||
| Enabling the use of stadiums and other spaces | 34 | 34 | 46 | 44 | 4 | 14 | 16 | |||||||||||||
| Increasing supplies (masks, ventilators) | 56 | 51 | 40 | 46 | 32 | 2 | 16 | -24 | 7 | 1 | ||||||||||
| Investment in vaccines and research | 28 | 39 | 46 | 46 | 34 | 15 | 6 | |||||||||||||
| Increasing care staff (volunteers, students, retirees, foreigners, humanitarian aid) | 46 | 44 | 46 | 47 | 19 | -2 | -24 | |||||||||||||
| Training for doctors | 22 | 44 | ||||||||||||||||||
| Incentives (monetary) for care staff | 52 | 47 | 17 | |||||||||||||||||
| Strategies for population at risk | ||||||||||||||||||||
| Special conditions for over 70 years old people or children | 41 | 45 | 38 | 36 | 12 | 12 | 12 | |||||||||||||
| Special measures for population deprived of liberty | 41 | 18 | 18 | |||||||||||||||||
| Raising isolation measures for cases of domestic violence | 40 | 17 | ||||||||||||||||||
| Limiting access to care facilities or hospitals for the elderly | 54 | 49 | 46 | 10 | 18 | 12 | ||||||||||||||
| Social support | ||||||||||||||||||||
| Direct support with financial resources (bonds or other measures) | 50 | 53 | 51 | 41 | 32 | 48 | 15 | 14 | 18 | |||||||||||
| Tax or credit relief | 50 | 51 | 41 | 46 | 48 | 48 | 15 | 14 | 12 | 11 | ||||||||||
| Food support or other supplies for vulnerable people | 51 | 45 | 51 | 48 | 15 | 14 | 12 | |||||||||||||
| Labor or tenant protection measures (in order to avoid layoffs and evictions) | 42 | 46 | 46 | 18 | 15 | 17 | ||||||||||||||
| Improving payment conditions due to sickness or disability | 50 | 41 | 32 | 18 | 3 | |||||||||||||||
| Coordination of donations | 49 | 15 | ||||||||||||||||||
| ONG participation | 41 | -347 | ||||||||||||||||||
| Interventions to endorse goods and services production | ||||||||||||||||||||
| Direct support with financial resources for companies | 55 | 63 | 53 | 51 | 46 | 40 | 18 | 15 | 21 | |||||||||||
| Tax and credit reliefs and facilitating loans to companies | 55 | 50 | 53 | 51 | 46 | 47 | 48 | 18 | 15 | 21 | ||||||||||
| Economic plans | 55 | 51 | 56 | 46 | 48 | 18 | 15 | 21 | ||||||||||||
| Food and drug supply plans | 40 | 45 | 15 | 14 | ||||||||||||||||
| Regulation of medicine retail price | 41 | 21 | ||||||||||||||||||
| Information, communication, and endorsement to social distancing | ||||||||||||||||||||
| Mobile apps with information | 30 | 6 | 16 | 20 | 4 | -15 | ||||||||||||||
| Daily media reports | 6 | 53 | 49 | 43 | -24 | -32 | 6 | |||||||||||||
| Educational campaigns | 21 | 42 | 48 | 44 | 30 | 32 | 14 | -24 | -32 | |||||||||||
| Publiccation of plans, decrees, recommendations on specific | 53 | 43 | 38 | 28 | -41 | -32 | -7 | |||||||||||||
| National increase in internet speed for all users | 17 | |||||||||||||||||||
| Enabling free call lines for nationals abroad | 5 | 14 | 10 | |||||||||||||||||
| Promoting remote working or telemedine | 55 | 42 | 38 | 15 | 13 | 8 | ||||||||||||||
Appendix 3.
Appendix 3. Key findings of studies that addressed the impact of non-pharmaceutical interventions.
| Non-pharmacological interventions | Impact | Findings |
|---|---|---|
| Combination of measures | High | Two modeling studies (SIR) of COVID-19 infection stablished that strict prevention and early control measures, such as quarantine, social distancing or detention of public transportation service, reduce the infection’s contact rate and efficiency, and therefore, are the key on the outbreak. (11) |
| Non-pharmacological measures such as restriction of travels between cities, social distancing and contact reduction, as well as early detection and isolation, have made a substantial reduction of the COVID-19’s transmission in Chine. It is estimated that early detection and isolation of the positive cases prevent more infection than restriction in traveling and contact reduction (5 5 versus 2.6 times), but non-pharmacological measures all integrates made the strongest and fastest effect. (12) | ||
| Without the implementation of non-pharmacological measures, case numbers of COVID-19 would have increased rapidly in China, 51 times in Wuhan, 92 times in other cities from Hubei and 125 times in other provinces. (12) | ||
| Implementation times of intervention are also critical. Case’s numbers can be drastically reduced in 66%, 86% and 95%, respectively, if NPI could be driven in a week, two week and three weeks before the real time in which they were implemented on the whole country. Also, geographic range of affected areas can be reduced from 308 to 192, 130 and 61 cities, respectively. (12) | ||
| On most scenarios, tracking of contacts is highly effective and the isolation of positive cases it’s enough to control new outbreaks for COVID-19 in three months. Control probability decreases with long delays from the beginning of symptoms to isolation, can determined less cases from contact tracking and increases the transmission before symptoms. (13) | ||
| The effectiveness of any isolated intervention can be limited, which requires combination of multiple interventions to have a substantial impact on transmission. (10) | ||
| Optimal mitigation policies (which combine home isolation of suspicious cases, home quarantine of the people who live in the same place as the suspicious case and social distancing of elderly and people at higher risk of severe illness) may reduce the maximum demand of medical care and mortality between 2/3 and a half However, resulting mitigated pandemic probably would lead to hundreds of thousands of deaths and collapsed health services. (10) | ||
| In total, on a non-mitigated pandemic, we can predict approximately 510.000 deaths in UK and 2.2 million in USA, without taking into account the possible negative effects of a collapsed health system. (10) | ||
| For a non-controlled epidemic, we can predict that the demand of ICU beds will be exceeded from the second week of April, with a peak in demand 30 times higher than de maximum offer in both countries. (10) | ||
| Cities that implement any combination of control measures preventively, before any case of COVID-19, informed 33.3% (IC 95%: 11.1-44.4%) less cases confirmed by laboratory during the first week of (13.0, IC 95%: 7.1-18.8, n = 125), compared with cities who started control measures later (20.6 cases, IC 95%: 14.5-26.8, n = 171; difference between groups, U = 8197 z = -3.4, P <0.01). (14) | ||
| Inside the specific control measures, cities who suspended public transportation within the city and/or closed entertaining places and forbidden public reunions, and made it before, informed less cases during the first week of outbreak. (14) | ||
| Case isolation | High | It is estimated that early detection and isolation of cases prevent more infection tan traveling restriction and contact reduction (5 vs 2.6 times), but non-pharmacological measurements all together have a stronger and faster impact. (12) |
| Early detection of cases | High | It is estimated that early detection and isolation of cases prevent more infection tan traveling restriction and contact reduction (5 vs 2.6 times), but non-pharmacological measurements all together have a stronger and faster impact. (12) |
| Contact tracking | High | On most scenarios, tracking of contacts is highly effective and the isolation of positive cases is enough to control new outbreaks for COVID-19 in three months. Control probability decreases with long delays from the beginning of symptoms to isolation, can determined less cases from contact tracking and increases the transmission before symptoms. (13) |
| Quarantine of contacts | High | Four cohort studies and 15 modeling studies of SARS (Severe acute respiratory syndrome) and MERS (Middle east respiratory syndrome) confirmed the effectiveness of quarantine on individuals that have had close contact with confirmed cases. (11) |
| Only three studies considered the effectiveness of quarantine on hypothetical examples that also modeled the pre-symptomatic infectiousness. The studies are consistent on identifying that quarantine effectiveness depends on a critical way from the biological dynamics of the infectious disease (for example, latent periods and infectious periods) and transmissibility. When the transmissibility is relatively low (basic reproductive number <2.5), the quarantine may control a disease, even when the infectiousness precedes the symptoms for several days. When transmissibility is high and symptoms come many days after infectiousness, quarantine may be enough. (11) | ||
| The related evidence with flu pandemics indicates that quarantine of exposed people may delay the peak on local epidemics during the first stages of it, which helps reducing the disease load and also delays the propagation. ECDC | ||
| A 14 days quarantine is considered enough to control contact cases of COVID-19, quick identification of cases increases the effectiveness of quarantine measurement. (15) | ||
| Public transportation suspension | High | In Wuhan, if they haven’t stablished any traveling restriction on January 23th, cases may have been increased in 118 % (91% -172%), which leads to 13,857 more cases (10,920-20,574), if the prohibition haven’t been decreed three days before, it may have reduced cases in 47% (26% -58%), which involves 3,103 less cases (1,732-3,820), cases would have been reduced on a 83% (78% -89%) if this measure would have been taken a week before. (16) |
| Cancelling public meetings | High | Data from seasonal influenza models and pandemic influenza models indicates that, during mitigation stage, cancelling public massive meetings before the epidemic peak may reduce virus transmission. (15) |
| A systematic review from 24 studies found Little but consistent evidence on the fact that influenza transmission occurs among pilgrims on main religious events. Main sports events such as Olympic Games and World Football Cup, detected a marginal increase on incidence of all the infectious diseases, including the flu, with infections limited to competitors and the staff, instead of the crowds or the general community. (17) | ||
| Maintenance of social distancing measures, (at least six months after outbreak) | High | If the contact with the population resume to normal levels observed on previous years, the suspension on traveling restriction may produce an increasing on the epidemic. Thus, the social distancing may continue during several months. (12) |
| The main challenge in the suppression is that the package of intensive intervention, or something equivalent, effective to reduce the transmission, may be maintained until a vaccine is available (potentially 18 months or so), because it has been predicted that transmission may recover fast if we relax the measures. (10) | ||
| Self-isolation of symptomatic patients | Moderate-High | Self-isolation of individuals with respiratory infection symptoms in one of the most important measures to reduce transmission of diseases and limit the spread of virus on the community during an epidemic. (15) |
| Social distancing of people older than 70 years | Moderate | Studies have always considered the contact reduction along with other non-pharmacological measures, (12) |
| Working areas measurements | Moderate | Measures on workplaces (flexible work schedules/shifts for employees, telecommuting, physical distancing) are recommended on people with acute respiratory diseases. (15) |
| Social distancing | Low- Moderate | Studies have always considered social distancing along with other non-pharmacological measurements. (10-12) |
| Restriction of travels between cities | Low- Moderate | Warnings to not travel during epidemics have the goal of reducing the number of infected people during the trip to areas or countries where community transmission is in progress: reducing import risk from affected countries and reducing the transmission among travelers (for example, the line son airport and on airplanes) (15) |
| Restriction of domestic flights | Low- Moderate | General restrictions of domestic travels can have a small positive impact on delaying an epidemic, only if they are implemented on early stages. Such restrictions may be considered only during contention stage of a high severity epidemic. (15) |
| While we couldn’t contain a higher propagation f COVID-19, attributed measures to Hubei blocking helped reduced the infection speed and reduce the correlation of national air traffic with COVID-19 cases within China, while interpreting changes observed in time of duplication, may be considered all measures imposed at Wuhan. Data cannot make difference between which strict measures succeeded the most, because the analysis only evaluated the effectiveness of the whole measures. All measures were partially successful and have resulted on delayed propagation of COVID-19 in China. (18) | ||
| Travel ban from Wuhan delayed the arrival time of COVID-19 to other cities in an average of 2.91 days (IC 95%: 2.54-3.29 days). More than 130 cities, covering more than half of China's geographic area and population, benefited from the delay. This delay provided additional time to prepare for the arrival of COVID-19 in China but would not have stopped transmission after the infection was exported to new locations from Wuhan. (14) | ||
| Closing day-cares and schools (low impact) | Low- Moderate | Proactive school and daycare closing may be associated with significate cost to society and economy. During contention stage, school closing is not justified. There is no data that back up decision making on proactive school closing in terms of anticipated effectiveness to mitigate COVID-19 epidemic, due to de unknown transmission level of this virus on children. (15) |
| Quarentine of travelers from affectes areas | Low | Infection and death numbers avoided with quarantine of travelers from countries with declared outbreaks is substantially lower than quarantine of suspicions or contact cases. (11) |
| A retrospective cohort study and three modeling studies addressed the effectiveness of quarantine to reduce the transmission from individuals who travelled from high transmission rate areas One of the studies considered evidence of SAR outbreak on 2003 in Taiwan. Results of model show that in the hypothetical scenario where no one would have been quarantined after arriving from a high transmission rate region, there would be 511 additional SARS cases and 70 additional deaths. On data bases, they could track 17 imported cases not quarantined (lost cases and cases before the quarantine implementation). If these 17 imported cases would have been quarantined, 280 SARS cases and 48 deaths may have been avoided. Of the more than 95,000 people in quarantine, only two developed SARS. If these two individuals would have not been quarantined, it may have produced 29 additional cases and 5 deaths. (11) | ||
| Contact reduction | Low | LStudies always considered the reduction of contact along with other non-pharmacological (12) |
| Border closure | Low | According to evidence from modeling studies, mainly related with influenza pandemic, border closure may delay the introduction of virus to a country only if they are full and quickly implemented during early stages, which is only plausible on specific contexts (for example, on small nations, isolated and islands). Therefore, available evidence does not back up the border closure measure that may cause important secondary effects social and economic disorders. (15) |
| Airport case detection procedures | Low | Even though some imported cases of COVID-19 have been detected through airport detection procedures, available evidence from all the reviewed publications and the unpublished modeled work made on the ECDC suggests that border control measures are not effective to delay or mitigate a pandemic. This due to the low sensibility of used systems to detect infections lowly symptomatic and its inability to detect cases during incubation stage. (15) |
References
- 1.The Humanitarian Data Exchange . Coronavirus COVID-19 Global Cases. OCHA services; 2020. [2020 Mar 23]. Available from: https://data.humdata.org/dataset/novel-coronavirus-2019-ncov-cases. [Google Scholar]
- 2.WHO . WHO Director-General´s opening remarks at the media briefing on COVID-19-11 March 2020. Geneva: Switzerland; 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 [Google Scholar]
- 3.Presidencia de la República . Declaración del estado de emergencia Colombia: Marzo 2017. Presidencia de la República; Colombia: 2020. pp. 1–16. [Google Scholar]
- 4.Ferguson NM, Laydon D, Nedjati-Gilani G, Imai N, Ainslie K, Baguelin M, et al. Impact of non-pharmaceutical interventions (Non-pharmaceutical interventions) to reduce COVID-19 mortality and healthcare demand. Imperial College London; 2020. pp. 20–20. [DOI] [Google Scholar]
- 5.European Centre for Disease Prevention and Control Guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of 2019-nCoV. 2020
- 6.Nunan D, Brassey J. What is the evidence for mass gatherings during global pandemics? A rapid summary of best-available evidence. Centre Evidence-Based Medicine: Nuffield Department of Primary Care Health Sciences University of Oxford, Trip Database; 2020. [Google Scholar]
- 7.Hossain MP, Junus A, Zhu X, Jia P, Wen T-H, Pfeiffer D, et al. The effects of border control and quarantine measures on global spread of COVID-19. medRxiv. 2020;(Preprint) doi: 10.1101/2020.03.13.20035261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.European Centre for Disease Prevention and Control . Considerations relating to social distancing measures in response to the COVID-19 epidemic Scope of this document Key points. Stockholm: ECDC; 2020. [Google Scholar]
- 9.Lai S, Ruktanonchai NW, Zhou L, Prosper O, Luo W, Floyd JR. Effect of non-pharmaceutical interventions for containing the COVID-19 outbreak in China. medRxiv. 2020;1(1):1–29. doi: 10.1101/2020.03.03.20029843. [DOI] [Google Scholar]
- 10.Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020;3099(20) doi: 10.1016/S1473-3099(20)30129-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhang C, Chen C, Shen W, Tang F, LEi H, Xie Y. Impact of population movement on the spread of 2019-nCoV in China. Lancet Infect Dis. 2020;Preprint:30–30. doi: 10.2139/ssrn.3546090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tian H, Liu Y, Li Y, Wu C-H, Chen B, Kraemer MUG. The impact of transmission control measures during the first 50 days of the COVID-19 epidemic in China medRxiv. Prepr. 2020;1(1):1–29. doi: 10.1101/2020.01.30.20019844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lau H, Khosrawipour V, Kocbach P, Mikolajczyk A, Schubert J, Bania J, et al. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J Travel Med. 2020;001(714) doi: 10.1093/jtm/taaa037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Prem K, Liu Y, Russell T, Kucharski AJ, Eggo RM, Davies N, et al. The effect of control strategies that reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China. medRxiv. 2020;2667(20) doi: 10.1101/2020.03.09.20033050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chen W, Wang Q, Li YQ, Yu HL, Xia YY, Zhang ML, et al. Early containment strategies and core measures for prevention and control of novel coronavirus pneumonia in China. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(3):1–6. doi: 10.3760/cma.j.issn.0253-9624.2020.03.003. [DOI] [PubMed] [Google Scholar]
- 16.Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic. Lancet. 2020;2019(20):1–4. doi: 10.1016/S01406736(20)305675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Team Rs . RStudio: integrated development for R. RStudio, Inc; Boston, MA: 2015. http//www.rstudio.com [Google Scholar]
- 18.Gobierno de Mexico [2020 Mar 28];Informe técnico COVID-19 14 MARZO 2020. 2020 Available from: https://presidente.gob.mx/informe-tecnico-covid-19-14-marzo-2020/
- 19.KCDC Press Release: The updates on COVID-19 in Korea. 2020 2020 Mar 28; https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
- 20.Perfil . Nueva York y California, en cuarentena total por Covid-19. Perfil; 2020. https://www.perfil.com/noticias/internacional/nueva-york-y-california-en-cuarentena-total-por-covid-19.phtml [Google Scholar]
- 21.Nussbaumer-streit B, Chapman A, Dobrescu AI, Mayr V, Persad E, Klerings I. The effectiveness of quarantine to control the. Coronavirus disease. 2019:a–a. doi: 10.2139/ssrn.3550010. [DOI] [Google Scholar]
- 22.Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI, Russell TW, et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet. 2020;8(4):e488–e496. doi: 10.1016/S2214-109X(20)30074-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.González-jaramillo V, González-jaramillo N, Gómez-restrepo C, Palacio-acosta CA, Gómez-lópez A, Franco OH. Proyecciones de impacto de la pandemia COVID-19 en la población colombiana, según medidas de mitigación Datos preliminares de modelos epidemiológicos para el periodo del 18 de marzo al 18 de abril de 2020. Rev Salud Pública. 2020;(22):1–6. doi: 10.15446/rsap.V22n2.85789. [DOI] [PubMed] [Google Scholar]
- 24.Colbourn T. Comment COVID-19 : extending or relaxing distancing control measures. Lancet. 2020;2667(20):19–20. doi: 10.1016/S2468-2667(20)30072-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. Lancet. Preprint. 2020. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhang C, Deng H, Zhang Q. SSRN. 2019. The value of early response by surrounding areas of epidemic center hubei during COVID-2019 outbreak in china?: A quasi- experiment analysis; pp. 1–16. [DOI] [Google Scholar]
Colomb Med (Cali). 2020 Jun 30;51(2):e4266. [Article in Spanish]
Contribución del estudio
| 1) ¿Por qué se realizó este estudio? |
| Para saber qué intervenciones no farmacológicas (INFs) han adoptado diferentes países para la contención, mitigación o supresión de la pandemia de COVID-19 y en qué momento se implementaron. Para revisar la evidencia sobre el impacto de las intervenciones no farmacológicas en la contención, mitigación o supresión de la pandemia. |
| 2) ¿Cuáles fueron los resultados más relevantes del estudio? |
| Algunos países se centran en establecer restricciones de viaje, aislamiento de casos identificados y personas de alto riesgo. Otros tienen una combinación más intensa de medidas drásticas de distanciamiento social, como medidas de confinamiento obligatorias para toda la población y cierre de todos los centros educativos. Algunos de los países han implementado medidas drásticas de distanciamiento social en los primeros quince días después de la detección del primer caso, otros países han tardado más de 30 días. La efectividad de intervenciones no farmacológicas aisladas puede ser limitada, pero la combinación de intervenciones ha demostrado tener un alto impacto en la reducción de la transmisibilidad de la enfermedad, el colapso de los servicios de atención médica y la mortalidad. Cuando se ha controlado el número de casos nuevos, es necesario mantener medidas de distanciamiento social. La realización de pruebas, el rastreo de contactos y la cuarentena de los casos sospechosos podrían ser las principales estrategias para realizar después de que se hayan relajado las intervenciones no farmacológicas de distanciamiento social drástico. |
| 3) ¿Qué aportan estos resultados? |
| La evidencia sintetizada podría informar la toma de decisiones políticas con respecto al control de la enfermedad COVID-19. |
Introducción
La enfermedad por coronavirus 2019 (COVID-19) es una nueva enfermedad infecciosa que emergió rápidamente y que constituye una importante amenaza para la salud global 1. El 30 de enero de 2020, la Organización Mundial de la Salud (OMS) declaró el brote como una emergencia de salud global 2, mientras que Colombia lo hizo el 12 de marzo 3.
El virus SARS-CoV-2 parece tener una alta transmisibilidad, en ausencia de cuarentena completa y medidas de distanciamiento social el número de reproducción básica (R0) varía de 2.8 a 5.5, en comparación con el R0 promedio para los virus de influenza estacional que es en promedio 1,8 4.
En experiencias pasadas, como en la pandemia de influenza H1N1 de 1918-19, no se tenía disponibilidad de intervenciones efectivas o vacunas para tratar o prevenir la enfermedad; Esto nos enseñó que, bajo estas circunstancias, una variedad de intervenciones no farmacológicas (INFs) tienen éxito en la reducción del número de casos 4. Las INFs incluyen el aislamiento de personas enfermas, el rastreo de contactos, la cuarentena de personas expuestas, el distanciamiento social, las restricciones de viaje, el cierre de escuelas, iglesias y lugares de trabajo, y la cancelación de eventos de reunión masivos 4-9. Estas intervenciones han demostrado ser formas efectivas de responder al brote cuando se implementan temprano en la epidemia 4-6. Las epidemias pasadas también han demostrado que, si las intervenciones se mantienen, la mortalidad se reduce; sin embargo, "la transmisión se recupera una vez que se levantan los controles" 4.
Se han reconocido tres grupos de estrategias de intervención no farmacológicas, 1) contención, 2) mitigación y 3) supresión 6,7. Las intervenciones de contención son aquellas implementadas cuando se detectan los primeros casos con el fin de interrumpir la transmisión de la enfermedad, prevenir su propagación y dar tiempo al sistema de salud para hacer los preparativos para atender a los pacientes y esperar el desarrollo de vacunas e intervenciones efectivas 9. Las intervenciones de mitigación se utilizan cuando aumenta el número de casos y la posibilidad de encontrar una relación entre los casos es complicada, la mitigación no tiene como objetivo interrumpir la transmisión por completo, sino reducir el impacto en la salud de una epidemia sobre la mortalidad y el colapso del sistema de salud. 4,10. Y la supresión tiene la intención de reducir el número promedio de casos secundarios que cada caso genera 4.
Según el Imperial College, la supresión conlleva enormes costos sociales y económicos, que pueden tener por si mismos un impacto significativo en la salud y el bienestar a corto y largo plazo. La mitigación nunca podrá proteger por completo a las personas en riesgo de enfermedad grave o muerte y, por lo tanto, la mortalidad resultante puede seguir siendo alta 4.
En China, se han implementado tres importantes intervenciones no farmacológicas para controlar la propagación y reducir el tamaño del brote de COVID-19 9. Primero, las prohibiciones de viajes entre ciudades y el establecimiento de un cordón sanitario en Wuhan y las ciudades circundantes de la provincia de Hubei 9,11-13. En segundo lugar, medidas para mejorar la detección, el rastreo de contactos, la identificación, el diagnóstico, el aislamiento y la notificación de personas con sospecha de enfermedad y casos confirmados 9,14. Y tercero, la implementación de restricciones de viaje y de contacto al interior de la ciudad, las cuales incluyeron limitar el contacto social individual, el uso de medidas de higiene personal y de protección, y el aumento de la distancia física entre los que tienen COVID-19 y los que no 9,15. El gobierno chino también incito a las personas a quedarse en casa tanto como fuera posible, canceló o pospuso grandes eventos públicos y reuniones masivas, y cerró bibliotecas, museos y lugares de trabajo. 8,9.
La propagación progresiva de la enfermedad ha permitido a muchos países anticipar que se aproxima una pandemia 9,16. En el caso de Colombia, algunos gobiernos locales, así como el gobierno nacional, implementaron rápida y drásticamente un confinamiento obligatorio en todo el territorio nacional, así como otras intervenciones no farmacológicas dirigidas a la contención, supresión y mitigación de la enfermedad COVID-19.
Se requiere la mejor evidencia científica disponible para diseñar intervenciones no farmacológicas efectivas y difundir el conocimiento de manera urgente para ayudar a los tomadores de decisión a evaluar los posibles beneficios y costos de las intervenciones no farmacológicas para contener los brotes de COVID-19. Es esencial describir cómo diferentes países implementan intervenciones no farmacológicas y en qué punto de la epidemia. También es necesario explorar cómo esas intervenciones han impactado el número de casos, la mortalidad y la capacidad instalada de atención médica para prestar servicios de salud. Sin embargo, todavía hay brechas en el conocimiento sobre la efectividad de las diferentes intervenciones para justificar adecuadamente la preparación, implementación o cancelación de varias intervenciones no farmacológicas.
Materiales y métodos
Se realizó una síntesis rápida de evidencia enfocada en identificar las intervenciones no farmacológicas implementadas en la ciudad de Wuhan y 19 países (Argentina, Australia, Brasil, Canadá, Chile, China, Colombia, Cuba, Alemania, Irán, Italia, Japón, México, Noruega, Rusia, Corea del Sur, España, Reino Unido y Estados Unidos). Se aplicaron tres criterios para seleccionar los países y territorios, 1) un número comparativamente alto de casos, 2) una particularidad política o social que permita la comprensión de diferentes tipos de intervenciones no farmacológicas o un ritmo diferente en su implementación; y 3) un equilibrio entre países de Europa, Asia y América del Norte, Central y del Sur.
Se realizaron búsquedas en ocho páginas web de organizaciones transnacionales, 17 páginas web de revistas y periódicos internacionales y 99 páginas web de instituciones gubernamentales en los 19 países incluidos entre el periodo del 1 de enero al 25 de marzo de 2020. Además, se realizaron búsquedas en las bases de datos Medline y Embase de estudios que evaluaran la efectividad de las intervenciones no farmacológicas para la contención, supresión y mitigación de COVID-19 (Anexo 1 con las fuentes de búsqueda).
Se utilizaron documentos oficiales y artículos de medios de comunicación para determinar la fecha en que diferentes países implementaron las intervenciones no farmacológicas. Los criterios de elegibilidad de los artículos académicos fueron que el artículo se enfocara en explorar la efectividad y el impacto de las intervenciones no farmacológicas en la contención, supresión o mitigación de COVID-19, sin restricciones en lenguaje, o diseño del estudio. Los estudios elegibles incluyeron estudios observacionales (cohortes, series de tiempo, reportes de series), estudios de simulación y guías del sistema de salud o del sistema político.
La evaluación de la calidad de los estudios observacionales se realizó con los criterios de evaluación de Johana Briggs. En contraste, la calidad de los estudios de simulación no fue evaluada formalmente. Aun así, se emitió un juicio de acuerdo con la pertinencia de las variables utilizadas para realizar la simulación, la solidez de los supuestos y la calidad de la descripción del procedimiento estadístico. Todas las etapas del proceso de revisión fueron realizadas por un investigador y verificadas por un segundo investigador.
La información sobre el número de nuevos casos y muertes causadas por COVID-19 en los países y territorios elegidos se obtuvo del John Hopkins Center for Systems Science and Engineering después de notarse que sus tablas tienen información más actualizada que los informes de situación de la OMS 1. El primer caso reportado en cada país fue documentado de fuentes oficiales o de la OMS, con esta información, determinamos cuántos días transcurrieron entre el primer caso reportado y la decisión de la INF tomada por el gobierno. El número de días para tomar la decisión se utilizó para desarrollar una línea de tiempo de eventos, un mapa de calor y una figura conjunta que representa los nuevos casos día a día y el punto en el que se decidieron las intervenciones no farmacológicas. El mapa de calor se desarrolló con el software R 17.
Resultados
Todos los países han implementado varias intervenciones no farmacológicas para controlar la infección por COVID-19. Sin embargo, existe una variabilidad en la cantidad y tipo de intervenciones. En países como Brasil, Canadá, México y Rusia, identificamos pocas intervenciones, y ninguna de ellas estaba entre las medidas más drásticas de distanciamiento social, por ejemplo, México solo ha implementado el cierre de escuelas y universidades 18. Estos países se han centrado principalmente en evitar la entrada de casos utilizando restricciones de viajes y aislando los casos identificados y las personas de alto riesgo.
Otro grupo de países ha aplicado varias intervenciones, incluyendo alguna de las medidas drásticas de distanciamiento social. Corea del Sur, Reino Unido y Estados Unidos, por ejemplo, han implementado intervenciones de distanciamiento social más drásticas combinadas con realización de pruebas de detección, localización de contactos y aislamiento de casos y contactos. Cabe destacar que Corea del Sur es reconocida por la rápida implementación de una estrategia de detección de casos en masiva 19, mientras que solo recientemente en algunos de los estados de Estados Unidos se ha comenzado a implementar medidas de distanciamiento social 20.
El tercer grupo de países ha aplicado una combinación intensa de intervenciones drásticas para la contención, mitigación y supresión de la infección. Argentina, Chile, China, Colombia, Italia, España, todos implementaron confinamiento obligatorio para toda la población, después de cerrar escuelas y universidades, cancelar todos los eventos que concentraran a más de 200 personas y suspender el transporte público para todos los que no realizan trabajos esenciales para el control de la infección. Además, también han empleado aislamiento de casos y rastreo de contactos, cierre de fronteras y algunos están implementando la detección masiva de casos.
Con respecto al ritmo de implementación de las estrategias, algunos países como Argentina, Chile y Colombia, que reportaron el primer caso en marzo, implementaron intervenciones en los primeros quince días después de la detección del primer caso (Tabla 1 para más detalles), o incluso antes de la notificación del primer caso, como es el caso de Chile. Argentina, Chile y Colombia han tenido la oportunidad de anticipar y aprender de las decisiones políticas tomadas en otros países, como China y Corea del Sur, afectados desde diciembre de 2019 y enero de 2020 (Figura 1 que muestra un mapa de calor del momento para implementar las intervenciones). Países como Italia, España y Estados Unidos tardaron más de 30 días en implementar medidas drásticas de distanciamiento social y están mostrando una situación extrema de colapso de sus sistemas de salud (Figura 2 información sobre el momento en el cual algunos países han implementado algunas decisiones y la cantidad de casos nuevos que tenían en ese momento).
Tabla 1. Intervenciones no farmacologicas y número de días para implementarlas después del primer caso de COVID-19 (hasta el 28 de marzo de 2020).
| Paises/ fecha primer caso | Hubei | China | Japón | Corea del Sur | Estados Unidos | Australia | Canadá | Alemania | España | Italia | Rusia | Reino Unido | Irán | Brasil | Noruega | México | Chile | Argentina | Colombia | Cuba |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 31/12/19 | 31/12/2019 | 15/01/20 | 20/01/20 | 21/01/20 | 26/01/20 | 27/01/20 | 27/01/20 | 31/01/20 | 31/01/20 | 1/02/20 | 1/02/20 | 20/02/20 | 26/02/20 | 27/02/20 | 29/02/20 | 3/03/20 | 3/03/20 | 6/03/20 | 13/03/20 | |
| Medidas | ||||||||||||||||||||
| Declaración de emergencia | 23 | 13 | 52 | 53 | 43 | 9 | 25 | -24 | 9 | 6 | ||||||||||
| Distanciamiento social a nivel poblacional | ||||||||||||||||||||
| Cuarentena obligatoria en todo el territorio | 23 | 24 | 62* | 59 | 38 | 52 | 18 | 16 | 16 | |||||||||||
| Suspender clases presenciales | 23 | 48 | 43 | 41 | 30 | 5 | 14 | 14 | 12 | 12 | 10 | 11 | ||||||||
| Suspender concentraciones de personas | 20 | 54 | 43 | 39 | 39 | 14 | 15 | 14 | 6 | |||||||||||
| Suspensión del transporte público | 23 | 41 | 51 | 35 | 14 | |||||||||||||||
| Aislamiento de casos o contactos | ||||||||||||||||||||
| Aislamiento por llegar desde China | 20 | 50 | 2 | 34 | -18 | -41 | -26 | 4 | ||||||||||||
| Aislamiento por llegar desde otro país | 62 | 49 | 58 | 33 | 34 | 15 | 3 | 3 | 4 | 7 | ||||||||||
| Aislamiento por ser persona de alto riesgo | 46 | 34 | 53 | 38 | 49 | 18 | 16 | 19 | 14 | 12 | -45 | |||||||||
| Aislamiento por tener síntomas o ser un caso | 31 | 46 | 40 | 14 | 18 | -41 | 8 | |||||||||||||
| Restricciones de viaje | ||||||||||||||||||||
| Restricciones de entrada a extranjeros (China) | 19 | 2 | 10 | 54 | 49 | 30 | -1 | 14 | -46 | 14 | 9 | 9 | ||||||||
| Restricciones de entrada a extranjeros (otros) | 61 | 59 | 39 | 54 | 49 | 43 | 39 | 27 | 22 | 16 | 15 | 14 | 12 | 9 | ||||||
| Cierre de frontera para tráfico no esencial | 57 | 54 | 51 | 51 | 44 | 26 | 14 | 15 | 13 | 10 | 7 | |||||||||
| Restricciones de viajes internacionales | 54 | 58 | 58 | 54 | 48 | 39 | 38 | 32 | 46 | 25 | 16 | 15 | 9 | |||||||
| Restricciones a viajes aéreos domésticos | 31 | 31 | 54 | 48 | 38 | 41 | 25 | 17 | 14 | 16 | ||||||||||
| Detección y rastreo de casos | ||||||||||||||||||||
| Búsqueda intensiva de casos (En puerto de entrada y en territorios/provincias) | 20 | 21 | 6 | 6 | 19 | 44 | 5 | 8 | -32 | 5 | ||||||||||
| Rastreo de contactos | 20 | 21 | 33 | 6 | 10 | -41 | 10 | |||||||||||||
Figura 1. Mapa de calor de las intervenciones no farmacológicas y número de días en que se implementaron después del primer caso de COVID-19.
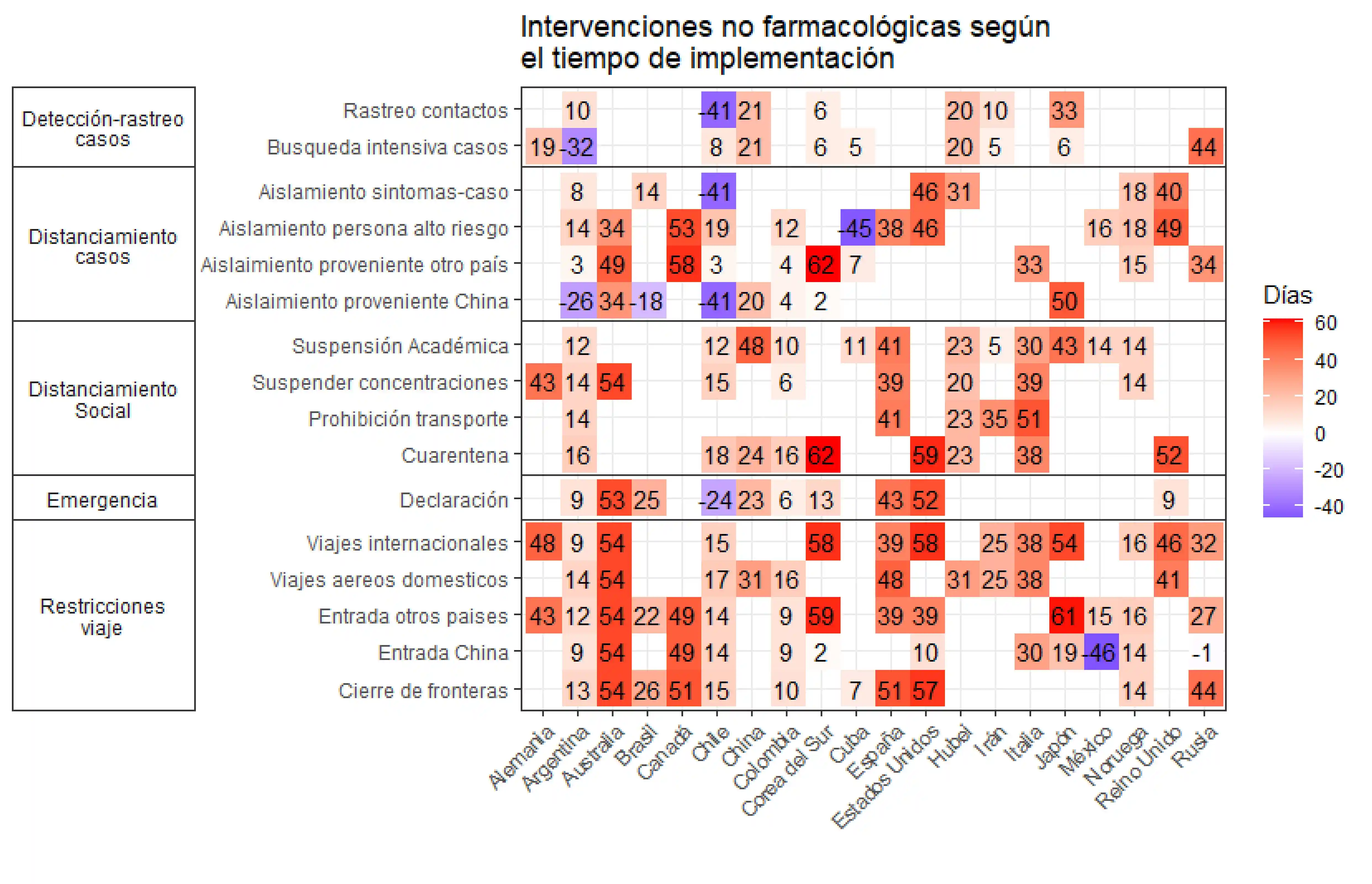
Figura 2. Número de casos nuevos de COVID-19 y día de implementación de algunas intervenciones no farmacológicas .
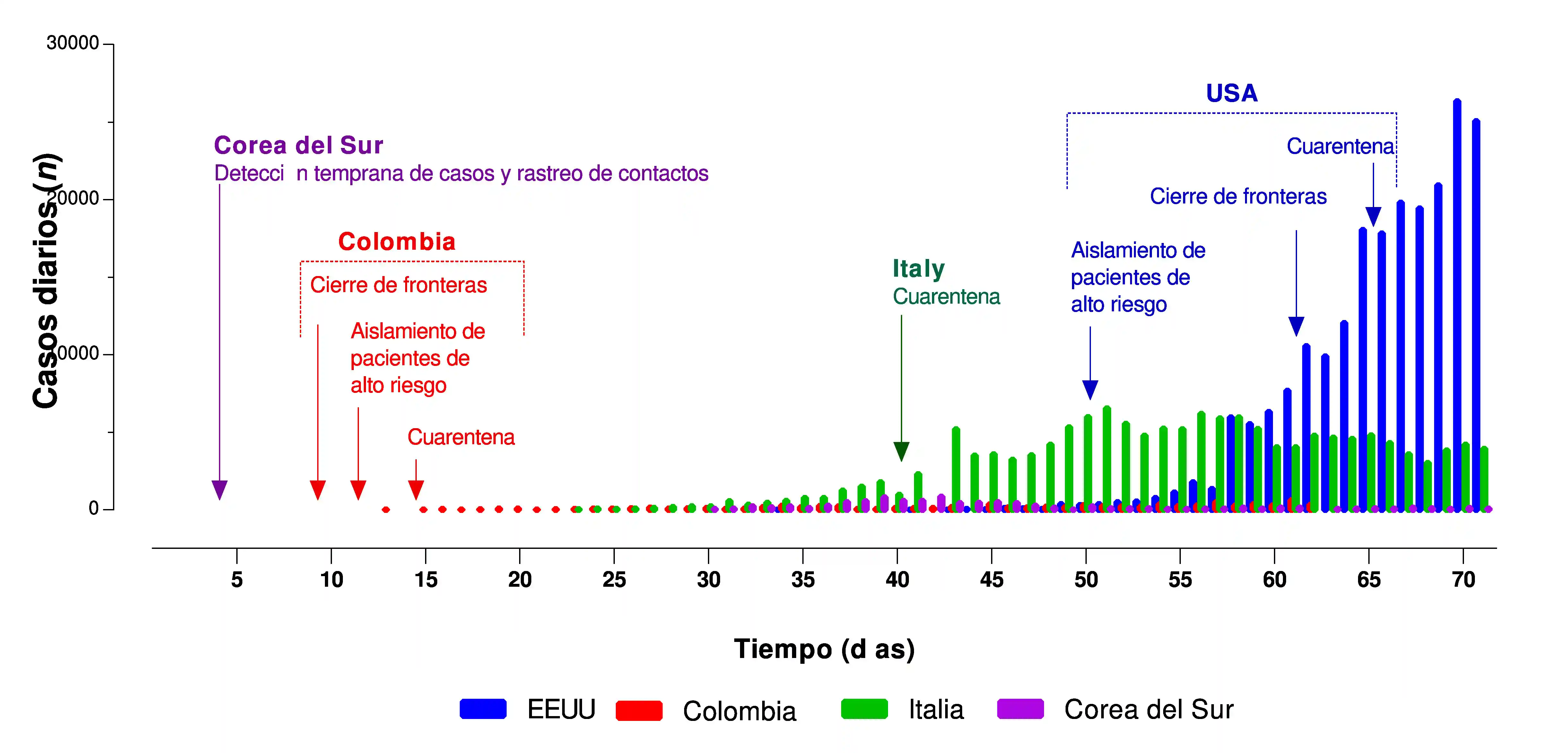
Otras intervenciones no farmacológicas implementadas por los países analizados incluyen intervenciones para mejorar la infraestructura del sistema de salud y fortalecer la capacidad de recurso humano (p. ej., ampliar la capacidad de camas, habilitar el uso de estadios y otros espacios), estrategias dirigidas a las poblaciones en riesgo (p. ej., medidas especiales para las personas privadas de libertad), intervenciones de apoyo social (p. ej., ayudas tributarias), estrategias para apoyar la producción de bienes y servicios (p. ej., facilitar préstamos a empresas) y estrategias de información precisa, comunicación oportuna y apoyo para el distanciamiento social (Anexo 2).
Impacto de las intervenciones no farmacológicas
Al explorar la efectividad de las intervenciones no farmacológicas para la contención, supresión y mitigación de la infección por COVID-19, incluimos nueve de 34 estudios identificados (una guía de política, una revisión sistemática rápida, dos estudios de cohortes, un estudio de series de tiempo y cuatro simulaciones) 4-6,11-13,21,22. El anexo 3 resume los hallazgos de estos estudios.
La efectividad de cualquier intervención no farmacológica aislada puede ser limitada, pero las intervenciones combinadas han demostrado ser efectivas y tienen un alto impacto en la reducción de la transmisibilidad de la enfermedad, el colapso de los servicios de atención médica y la mortalidad. Siete de nueve estudios incluidos sugieren explícitamente la implementación temprana de intervenciones combinadas y estrictas; principalmente, cuarentena, distanciamiento social, suspensión del transporte público, detección temprana de casos y aislamiento domiciliario de casos leves 4,5,9,12,13,21,22 (Tabla 2).
Tabla 2. Impacto de las intervenciones no farmacológicas para el control de la infección por COVID-19.
| Medida no farmacológica | Impacto | Número de estudios que abordan la medida | Tipo de estudio |
|---|---|---|---|
| Combinación de medidas | Alto | 7 | 1 guía de política |
| 2 estudios de cohorte | |||
| 1 revisión sistemática rápida | |||
| 1 estudio de serie de tiempo | |||
| 2 simulaciones | |||
| Aislamiento de casos | Alto | 3 | 1 guía de política |
| 2 simulaciones | |||
| Detección temprana de casos | Alto | 2 | 1 guía de política |
| 1 simulación | |||
| Rastreo de contactos | Alto | 1 | 1 simulación |
| Cuarentena de contactos | Alto | 2 | 1 estudio de cohorte y 1 guía de política |
| Suspensión del transporte público | Alto | 2 | 1 revisión sistemática rápida |
| 1 estudio de cohorte | |||
| Cancelación de grandes reuniones | Alto | 2 | 1 guía de política |
| 1 estudio transversal | |||
| Sostenimiento de medidas de distanciamiento (al menos seis meses después del brote) | Alto | 2 | 2 simulaciones |
| Autoaislamiento de personas sintomáticas | Moderado-alto | 2 | 1 guía de política |
| 1 simulación | |||
| Distanciamiento social de los mayores de 70 años | Moderado | 1 | 1 simulación |
| Medidas en el lugar de trabajo | Moderado | 1 | 1 guía de política |
| Distanciamiento social | Bajo-Moderado | 3 | 2 simulaciones |
| 1 revisión sistemática rápida | |||
| Restricción de viaje entre ciudades | Bajo-Moderado | 2 | 1 guía de política |
| 1 simulación | |||
| Restricciones de viajes domésticos | Bajo-Moderado | 3 | 1 guía de política |
| 1 estudio de cohorte | |||
| 1 estudio transversal | |||
| Cierres de escuelas y guarderías (bajo impacto) | Bajo-Moderado | 2 | 1 guía de política |
| 1 simulación | |||
| Cuarentena de viajeros provenientes de zona afectada | Bajo | 1 | 1 estudio de cohorte |
| Reducción de contacto | Bajo | 1 | 1 estudio de simulación |
| Cierres de fronteras | Bajo | 1 | 1 guía de política |
| Procedimientos de detección de casos en aeropuertos | Bajo | 1 | 1 guía de política |
Un estudio en China afirma que, sin la implementación de intervenciones no farmacológicas, el número de casos de COVID-19 habría aumentado de 51 veces en Wuhan, 92 veces en otras ciudades de Hubei y 125 veces en otras provincias 9. Las intervenciones no farmacológicas combinadas podrían reducir la demanda máxima de atención médica y la mortalidad a la mitad o incluso a dos tercios 4. Un estudio de simulación para el Reino Unido y los Estados Unidos muestra que, en una epidemia no controlada, la demanda de camas de cuidados intensivos se prevé que se vea excedida a partir de la segunda semana de abril, con una demanda máxima de camas de más de 30 veces el máximo suministro en ambos países 4.
Después del pico de la enfermedad, y cuando se ha controlado el número de casos nuevos, es necesario mantener medidas de distanciamiento social, control del transporte público, estrategias de trabajo en el hogar, detección y aislamiento de casos y rastreo de contactos. Se sugiere que el rastreo de contactos y el aislamiento de casos son altamente efectivos para controlar un nuevo brote de COVID-19. Sin embargo, la probabilidad de control disminuye con 1) largos retrasos desde el inicio de los síntomas hasta decidir el aislamiento, 2) pocos contactos rastreados por caso y 3) cuando aumenta la transmisión antes de los síntomas 22. En la mayoría de los escenarios de simulación y de la experiencia de salud pública de epidemias anteriores, se identifica que, si el contacto social se reanuda a niveles normales, los contagios podrían aumentar nuevamente. Por lo tanto, varias intervenciones no farmacológicas, incluido el distanciamiento social, deben continuarse durante varios meses, 9 incluso se propone que se mantengan medidas restrictivas hasta que haya una vacuna disponible (potencialmente 18 meses o más) ya que se predice que la transmisión se recupere rápidamente si se flexibilizan las intervenciones 4.
Cuando el número de casos nuevos demuestra el control de la enfermedad, la evidencia sugiere que las medidas que se pueden levantar primero son el cierre de fronteras, los procedimientos de detección de casos en los aeropuertos y el cierre de escuelas y guarderías. La evidencia también sugiere que tanto el establecimiento como la eliminación de intervenciones no farmacológicas dependen de varios factores políticos, sociales y culturales, no solo del comportamiento de la enfermedad 5,9,21.
Discusión
Resumen de los hallazgos principales
Consultamos ocho páginas web de organizaciones transnacionales, 17 de medios internacionales, 99 de instituciones gubernamentales en los 19 países incluidos, y, además incluimos nueve estudios (de 34 identificados) que cumplían con los criterios de inclusión. Encontramos que algunos países se centran en establecer restricciones de viaje, aislamiento de casos identificados y personas de alto riesgo. Otros tienen una combinación más intensa de confinamiento obligatorio para toda la población, cierre de todos los centros educativos y suspensión del transporte público para todos aquellos que no realicen trabajos esenciales. Algunos de los países han implementado intervenciones en los primeros quince días después de detectar el primer caso, mientras que otros han tardado más de 30 días en implementar medidas drásticas de distanciamiento social. La efectividad de las intervenciones no farmacológicas aisladas puede ser limitada, pero las intervenciones combinadas han demostrado ser efectivas y tener un alto impacto en la reducción de la transmisibilidad de la enfermedad, el colapso de los servicios de atención médica y la mortalidad. Cuando se ha controlado el número de casos nuevos, es necesario mantener medidas de distanciamiento social, control del transporte público, estrategias de trabajo en el hogar, detección de casos, autoaislamiento y rastreo de contactos durante varios meses.
Comparación con otros estudios
Un estudio de simulación realizado en Colombia para predecir el impacto de la pandemia de COVID-19 de acuerdo con las medidas de mitigación que se han implementado en el país concuerda con nuestros hallazgos de que las intervenciones combinadas podrían ser efectivas y tener un alto impacto en la reducción de la transmisibilidad de la enfermedad. El estudio de González-Jaramillo et al. 23, concluye que la combinación de estrategias de mitigación adoptadas por el gobierno colombiano podría reducir el número de pacientes que requerirían unidades de cuidados intensivos de 36,782 en el escenario de no intervención a 1,176 en el escenario que combina aislamiento de casos, cuarentena domiciliaria y distanciamiento social de personas mayores de 70 años.
Nuestro hallazgo de la necesidad de mantener medidas de distanciamiento social, control del transporte público, estrategias de trabajo en el hogar, detección y aislamiento de casos y rastreo de contactos también ha sido respaldado en la literatura. El modelo desarrollado por Prem et al. 14, Sugiere que el levantamiento repentino de las intervenciones podría conducir a un pico secundario más temprano, que podría evitarse relajando las intervenciones gradualmente. En este sentido, Colburn sugiere que la realización de pruebas, el rastreo de contactos y la cuarentena de casos sospechosos podrían ser las estrategias principales después de la relajación de las intervenciones no farmacológicas de distanciamiento social drástico para prevenir la sobrecarga del sistema de salud. Colburn 24 llama a la incorporación de estas estrategias en modelos que permitan que los países tengan una mejor idea de la capacidad de realización de pruebas que necesitarán y a decidir si dichas políticas pudieran tener éxito en la supresión de la propagación de COVID-19 en un determinado país.
Las intervenciones no farmacológicas también tienen efectos adversos en los individuos, las comunidades y la economía nacional. Una revisión rápida reciente informó que la cuarentena podría tener efectos psicológicos nocivos, como síntomas de estrés postraumático, confusión e ira, que pueden conducir a efectos adversos psicológicos a largo plazo 21,25. Muchos artículos han destacado las implicaciones económicas que las intervenciones de cuarentena podrían tener sobre la economía en el año 2020; sin embargo, el objetivo en este momento es salvar tantas vidas como lo permitan nuestros recursos 4,5,8,9,12,13,21,26.
Limitaciones de esta revisión
Dadas las limitaciones de tiempo impuestas por el brote actual de coronavirus, tomamos algunas decisiones metodológicas críticas que deben considerarse. Un solo revisor aplicó los criterios de inclusión y la extracción de información de los estudios incluidos en esta síntesis. Además, la calidad de los estudios de simulación no fue evaluada formalmente.
Conclusión
En este momento la toma de decisiones políticas debe tener como objetivo optimizar las oportunidades de salvar vidas, reducir el colapso de los servicios de salud y minimizar el impacto económico y social sobre la población en general, pero principalmente sobre los más vulnerables. Es probable que el momento de implementar y levantar las intervenciones tenga un efecto sustancial en estos objetivos.
Anexo 1. Recursos de búsqueda.
WHO PAHO.
WHO Situation Dashboard. https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
WHO. 2019 Novel Coronavirus (2019nCoV): Strategic preparedness and response plan. 03 de Febrero. https://www.who.int/docs/default-source/coronaviruse/srp-04022020.pdf
Enfermedad por el Coronavirus (COVID-19). https://www.paho.org/es/temas/coronavirus/enfermedad-por-coronavirus-covid-19
UNION EUROPEA
Eurosurvelliance. https://www.eurosurveillance.org/content/eurosurveillance/browse
EU Commision COVID-19 Coronavirus data. https://data.europa.eu/euodp/en/data/dataset/covid-19-coronavirus-data/resource/62eb477f-be00-462a-831a-594095f7306a
Politico. Coronavirus in Europe https://www.politico.eu/coronavirus-in-europe/
ECDC. European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en
IATA. International Air Transport Association. Government Measures Related to Coronavirus (COVID-19). https://www.iata.org/en/programs/safety/health/diseases/government-measures-related-to-coronavirus/
Johns Hopkins University and Medicine. Coronavirus Resource Center. Interactive maps and news https://coronavirus.jhu.edu/
COVID-19 Expert Reality Check. Johns Hopkins Bloomberg School of Public Health. https://www.globalhealthnow.org/2020-02/coronavirus-expert-reality-check#quammen
Worldometer owned by Dadax. https://www.worldometers.info/coronavirus/
Evidence Aid https://www.evidenceaid.org/coronavirus-resources/
Otros medios de comunicación
Science Magazine. Mass testing, school closings, lockdowns: Countries pick tactics in ‘war’ against coronavirus. By Jon Cohen, Kai KupferschmidtMar. 18, 2020 , 11:30 AM. https://www.sciencemag.org/news/2020/03/mass-testing-school-closings-lockdowns-countries-pick-tactics-war-against-coronavirus
The Economist. The politics of pandemics. All governments will struggle. Some will struggle more than others. https://www.economist.com/leaders/2020/03/12/the-politics-of-pandemics
Prospect Magazine UK. Coronavirus: Why scientists are divided over the effectiveness of the UK’s strategy by Philip Ball / March 16, 2020. https://www.prospectmagazine.co.uk/science-and-technology/coronavirus-uk-herd-immunity-boris-johnson-government-plan-cure
StateNews. Understanding what works: How some countries are beating back the coronavirus by Helen Branswell March 20, 2020. https://www.statnews.com/2020/03/20/understanding-what-works-how-some-countries-are-beating-back-the-coronavirus/
The NY Times. The Coronavirus Outbreake https://www.nytimes.com/news-event/coronavirus?action=click&pgtype=Article&state=default&module=STYLN_coronahub&variant=show®ion=header&context=menu
Wikipedia . Resumen de decisiones de los gobiernos. https://en.wikipedia.org/wiki/National_responses_to_the_2019%E2%80%9320_coronavirus_pandemic
International restrictions https://en.wikipedia.org/wiki/Travel_restrictions_related_to_the_2019%E2%80%9320_coronavirus_pandemic
BBC News. Coronavirus pandemic. https://www.bbc.com/news/explainers
The Guardian. Coronavirus Outbreak. https://www.theguardian.com/world/coronavirus-outbreak
The Washington Post. Coronavirus news and maps. https://www.washingtonpost.com/world/2020/03/27/coronavirus-latest-news/
Aljazeera. Coronavirus Pandemic News. https://www.aljazeera.com/topics/events/coronavirus-outbreak.html
El Espectador. Coronavirus hoy: ¿Qué están haciendo otros países de América Latina para contener la pandemia?. https://www.elespectador.com/noticias/el-mundo/coronavirus-hoy-que-estan-haciendo-otros-paises-de-america-latina-para-contener-la-pandemia-articulo-910367
¿Qué está haciendo cada país de América Latina para frenar el nuevo coronavirus?. https://rpp.pe/mundo/actualidad/coronavirus-covid-19-que-esta-haciendo-cada-pais-de-america-latina-para-frenar-el-nuevo-coronavirus-noticia-1252868
Semana. Semana Tendencias Coronavirus. https://www.semana.com/noticias/coronavirus/126948
El Colombiano. Coronavirus en Colombia contra el miedo. https://www.elcolombiano.com/coronavirus-en-colombia-contra-el-miedo
Europapres. Agencia Europa Press https://www.europapress.es/
RFI. Noticias Coronavirus http://www.rfi.fr/es/tag/coronavirus/
CNN Noticias Coronavirus CNN https://cnnespanol.cnn.com/category/coronavirus.
Note: The following official sources and other media were consulted between March 16 and March 27 to identify the actions and strategies defined by the countries.
ALEMANIA
Fuentes Oficiales
Federal Ministry of Health. https://www.bundesgesundheitsministerium.de/en/press/2020/coronavirus.html#c17182
Robert Koch Institute. https://www.rki.de/EN/Home/homepage_node.html
The Federal Government. Together against Corona. https://www.zusammengegencorona.de/
Chancellor and Federal Government. https://www.bundesregierung.de/breg-en/search/998964!search
Otros medios de comunicación
Deutsche Welle. Coronavirus. https://www.dw.com/en/top-stories/coronavirus/s-32798
Coronavirus en Alemania: últimas noticias. https://www.deutschland.de/es/news/coronavirus-en-alemania-actualizaciones
Noticias Bundesliga. https://www.bundesliga.com/es/bundesliga/noticias/noticias-informacion-actualidad-liga-alemana-3034-2316
Pressemitteilungen. https://www.bundesgesundheitsministerium.de/presse/pressemitteilungen/2020/1-quartal/krisenstab-bmg-bmi-sitzung-5.html
Bundesministeriums für Verkehr und digitale Infrastruktur. https://www.bmvi.de/DE/Ministerium/Minister-Staatssekretaere/minister-staatssektretaere.html
Coronavirus: Jens Spahn trifft Gesundheitsminister der Länder. https://www.youtube.com/watch?v=nm5l-uxSeeM&feature=youtu.be
Statement von Jens Spahn bei Pressekonferenz vom 19.03.2020. https://www.youtube.com/watch?v=9dQKFImYaY0&feature=youtu.be
ARGENTINA
Fuentes Oficiales
Ministerio de Salud. Coronavirus. https://www.argentina.gob.ar/salud/coronavirus-COVID-19
Gobierno Nacional. Resumen de medidas. https://www.argentina.gob.ar/coronavirus/medidas-gobierno
Otros medios de comunicación
El Clarin. Coronavirus en Argentina: piden donaciones para ayudar a los que menos tienen https://www.clarin.com/sociedad/coronavirus-argentina-piden-donaciones-ayudar_0_9O4v1s5nJ.html
Infoabae. Argentina solo recibió ayuda de China para enfrentar la pandemia del coronavirus https://www.infobae.com/politica/2020/03/22/la-argentina-solo-recibio-ayuda-sanitaria-de-china-para-enfrentar-la-pandemia-del-coronavirus/
RSE Presente. En épocas de coronavirus una ONG contagia solidaridad. https://presenterse.com/en-epocas-de-coronavirus-una-ong-que-contagia-solidaridad/
AUSTRALIA
Fuentes Oficiales
Coronavirus: COVID-19: Western Australian Government response. https://www.wa.gov.au/organisation/department-of-the-premier-and-cabinet/coronavirus-covid-19-western-australian-government-response
Safe Work Australia. https://www.safeworkaustralia.gov.au/doc/coronavirus-covid-19-advice-employers
COVID-19 (Coronavirus) and the Australian border. https://www.homeaffairs.gov.au/news-media/current-alerts/novel-coronavirus
COVID-19 Coronavirus Information for Public Sector Employers. https://www.commerce.wa.gov.au/labour-relations/covid-19-coronavirus-information-public-sector-employers
Departamento de salud Gobierno de Australia https://www.health.gov.au/news
Health information for western Australia https://www.healthywa.wa.gov.au/Articles/A_E/COVID-clinics
Conferencia de prensa primer ministro de Australia https://www.pm.gov.au/media/transcript-press-conference
Actualización medidas primer ministro https://www.pm.gov.au/media/update-coronavirus-measures
Circular 5/2020 - Licencia COVID-19 y otras flexibilidades laborales. https://www.commerce.wa.gov.au/sites/default/files/atoms/files/pslr_circular_04_2020.pdf
BRASIL
Fuentes Oficiales
Agencia Nacional de Vigilancia Sanitaria. http://portal.anvisa.gov.br/
Ministerio de salud. https://www.saude.gov.br/noticias
Otros medios de comunicación
Infoabae. Brasil cerró sus fronteras a europeos y asiáticos por el coronavirus. https://www.infobae.com/america/america-latina/2020/03/20/brasil-cerro-sus-fronteras-a-europeos-y-asiaticos-por-el-coronavirus/
CANADÁ
Fuentes Oficiales
Public Health Agency of Canada. https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19.html
Página oficial Primer ministro. https://pm.gc.ca/
Página oficial- Gobierno de Canadá. https://www.canada.ca/
CHINA Y HUBEI
Fuentes Oficiales
Chinese Center for Disease Control and Prevention. http://www.chinacdc.cn/en/COVID19/
National Health Commission of the People's Republic of China. http://en.nhc.gov.cn/antivirusfight.html
CHILE
Fuentes Oficiales
Gobierno Nacional. Plan de Acción Coronavirus. https://www.gob.cl/coronavirus/
Ministerio de Salud. Seguimiento de casos. https://www.minsal.cl/nuevo-coronavirus-2019-ncov/casos-confirmados-en-chile-covid-19/
Ministerio de Relaciones Internacionales. Medidas. https://chile.gob.cl/chile/medidas-de-prevencion-ante-el-nuevo-coronavirus
Servicio Informativo del Instituto de Previsión Social. Ministerio del Trabajo. https://www.chileatiende.gob.cl/coronavirus
COLOMBIA
Fuentes Oficiales
Ministerio de Salud y Protección Social. Coronavirus. https://d2jsqrio60m94k.cloudfront.net/
Ministerio de salud. https://www.minsalud.gov.co/
Instituto Nacional de Salud. https://www.ins.gov.co/Noticias/Paginas/Coronavirus.aspx
Presidencia de la República. https://id.presidencia.gov.co
Ministerio de Transporte. https://www.mintransporte.gov.co
Aeronáutica Civil de Colombia. http://www.aerocivil.gov.co/
COREA DEL SUR
Korean Centers for Disease Control and Prevention. http://www.cdc.go.kr/board.es?mid=a30402000000&bid=0030
CUBA
Fuentes Oficiales
Presidencia de Cuba. Noticias y medidas. https://www.presidencia.gob.cu/es/noticias/
Ministerio de Comercio. Medidas coronavirus. https://www.mincin.gob.cu/content/medidas-de-protecci%C3%B3n-tomadas-en-el-sector-del-comercio-para-prevenir-cualquier-contagio-0
Ministerio Relaciones Internacionales. Medidas coronavirus. http://misiones.minrex.gob.cu/es/coronavirus
Ministerio de Salud Pública de la República de Cuba. https://salud.msp.gob.cu/
Otros medios de comunicación
Cibercuba. Mapa del Coronavirus en Cuba. https://www.cibercuba.com/tags/coronavirus-cuba
Infomed, Portal de la Red de Salud de Cuba. http://www.sld.cu/
ESPAÑA
Fuentes Oficiales
Alertas en Salud Pública de actualidad. MinSalud España. https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/home.htm
Instituto de Salud Carlos III. Situación de COVID-19 en España. https://covid19.isciii.es/
Portal de La Moncloa. https://www.lamoncloa.gob.es/Paginas/buscadoravanzado.aspx
Instituto de Mayores y Servicios Sociales. https://www.imserso.es/imserso_02/actualidad/2020/marzo/IM_130154
Ministerio del Interior no a Penitenciarias. www.interior.gob.es
Otros medios de comunicación
Lista de Medidas del gobierno de El Diario. https://www.eldiario.es
ESTADOS UNIDOS
Fuentes Oficiales
Centers for Disease Control and Prevention. https://www.cdc.gov/
Página oficial del coronavirus de CDC. https://www.coronavirus.gov
White house. https://www.whitehouse.gov/
Departamento de Estado. https://travel.state.gov/
Departamento de defensa. https://www.defense.gov/
Asociación de médicos de los Estados Unidos. https://www.ama-assn.org
Gobierno de los Estados Unidos. https://www.usa.gov/
ITALIA
Fuentes Oficiales
Ministero della Salute. Nuovo coronavirus. http://www.salute.gov.it/nuovocoronavirus
Ministero della Salute. Situazione in Italia. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5351&area=nuovoCoronavirus&menu=vuoto
Protezione Civile. Emergenza Coronavirus. http://www.protezionecivile.gov.it/
Instituto Superiore di Sanitá. http://www.iss.it/coronavirus
Trova norme salute. http://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73532
Guida per prevenire e affrontare lo stigma sociale. http://www.salute.gov.it/imgs/C_17_notizie_4149_0_file.pdf
Aeroporti di Roma. http://www.adr.it/it/web/guest/coronavirus
Governo Italiano Presidenza del Consiglio dei Ministri. http://www.governo.it/it/articolo/comunicato-stampa-del-consiglio-dei-ministri-n-33/14204
L'epidemiologia per la sanità pubblica Istituto Superiore di Sanità. https://www.epicentro.iss.it/
IRÁN
Fuentes Oficiales
Ministry of Health and Medical Education. News. http://irangov.ir/cat/509
Ayatollah Khamenei. Official website. http://english.khamenei.ir/
Otros medios de comunicación
Islamic Republic News Agency. https://en.irna.ir/ y https://es.irna.ir/
Iran Daily. http://www.iran-daily.com/
JAPÓN
Fuentes Oficiales
Ministry of Health, Labour and Welfare. About coronavirus Disease 2019. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html
Prime Minister of Japan and His Cabinet. Basic responses to COVID2019. http://japan.kantei.go.jp/ongoingtopics/coronavirus_info_e.html
MÉXICO
Fuentes Oficiales
Gobierno de México. Comunicados y decisiones. https://coronavirus.gob.mx/noticias/
Dirección General de Epidemiología. Mapa de casos. http://ncov.sinave.gob.mx/mapa.aspx
Sistema de Información de la Secretaría de Salud. http://sinaiscap.salud.gob.mx:8080/DGIS/
Instituto Mexicano del Seguro Social. http://www.imss.gob.mx/
Otros medios de comunicación
Diario AS México. Covid-19. https://mexico.as.com/tikitakas/tag/covid_19/a/
NORUEGA
Fuentes Oficiales
Norwegian Institute of Public Health. https://www.fhi.no/en/id/infectious-diseases/coronavirus/
Ministry of Health and Care Services. https://www.regjeringen.no/en/dep/hod/id421/
REINO UNIDO
Fuentes Oficiales
Government UK. Coronavirus. https://www.gov.uk/coronavirus
Coronavirus (COVID-19): UK government response. https://www.gov.uk/government/topical-events/coronavirus-covid-19-uk-government-response
The Health Protection (Coronavirus) Regulations 2020. http://www.legislation.gov.uk/uksi/2020/129/contents/made
Public Health England. https://www.gov.uk/government/organisations/public-health-england
Departamento de salud pública Inglaterra. https://www.gov.uk/government/organisations/department-of-health-and-social-care
Oficina del primer ministro. https://www.gov.uk/government/organisations/prime-ministers-office-10-downing-street
Ministerio de comunidades y gobierno local. https://www.gov.uk/government/organisations/ministry-of-housing-communities-and-local-government
Departamento de trabajo y pensiones. https://www.gov.uk/government/organisations/department-for-work-pensions
Departamento de negocios, energía e industria. https://www.gov.uk/government/organisations/department-for-business-energy-and-industrial-strategy
Portal Legislation.gov.co. http://www.legislation.gov.uk/ukpga/1984/22
Foreign Travel Advice. https://www.gov.uk/foreign-travel-advice
Foreign & Commonwealth Office. https://www.gov.uk/government/organisations/foreign-commonwealth-office
Noticias gobierno de UK. https://www.gov.uk/government/news/
Statutory Sick Pay. Pago estatutario de enfermedad. https://www.gov.uk/statutory-sick-pay
Portal de noticias NHS. https://www.england.nhs.uk/2020/03/nhs-111-online-to-help-people-with-coronavirus/
Anexo 2.
Anexo 2. Intervenciones no farmacológicas y número de días en los cuales fueron implementadas (Hasta marzo 28, 2020).
| Estrategias | Hubei | China | Japón | Corea del Sur | Estados Unidos | Australia | Canadá | Alemania | España | Italia | Rusia | Reino Unido | Irán | Brasil | Noruega | México | Chile | Argentina | Colombia | Cuba |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paises/fecha del primer caso | 31/12/19 | 31/12/2019 | 15/01/20 | 20/01/20 | 21/01/20 | 26/01/20 | 27/01/20 | 27/01/20 | 31/01/20 | 31/01/20 | 1/02/20 | 1/02/20 | 20/02/20 | 26/02/20 | 27/02/20 | 29/02/20 | 3/03/20 | 3/03/20 | 6/03/20 | 13/03/20 |
| Declaración de emergencia | 23 | 13 | 52 | 53 | 43 | 9 | 25 | -24 | 9 | 6 | ||||||||||
| Distanciamiento social a nivel poblacional | ||||||||||||||||||||
| Cuarentena obligatoria en todo el territorio (o en parte del territorio) | 23 | 24 | 62 | 59 | 38 | 52 | 18 | 16 | 16 | |||||||||||
| Suspender clases presenciales en jardines, colegios o universidades | 23 | 48 | 43 | 41 | 30 | 5 | 14 | 14 | 12 | 12 | 10 | 11 | ||||||||
| Cierre de cines, restaurantes, y otros lugares de encuentro social | 23 | 55 | 37 | 48 | 14 | 17 | 14 | 12 | ||||||||||||
| Cierre de parques públicos (incluidos museos) | 20 | 41 | 49 | 5 | 14 | 14 | 12 | |||||||||||||
| Suspender concentraciones de personas | 20 | 54 | 43 | 39 | 39 | 14 | 15 | 14 | 6 | |||||||||||
| Cierre de actividades no esenciales | 14 | 14 | ||||||||||||||||||
| Prohibición de la movilidad en medios de transporte públicos o privados | 23 | 41 | 51 | 35 | 14 | |||||||||||||||
| Distanciamiento social de casos o contactos | ||||||||||||||||||||
| Aislamiento por 14 por asistir a sitios de alta afluencia de personas | 4 | |||||||||||||||||||
| Aislamiento por llegar desde China | 20 | 50 | 2 | 34 | -18 | -41 | -26 | 4 | ||||||||||||
| Aislamiento por llegar desde otro país | 62 | 49 | 58 | 33 | 34 | 15 | 3 | 3 | 4 | 7 | ||||||||||
| Aislamiento por vivir con un posible caso | 14 | -41 | 14 | |||||||||||||||||
| Aislamiento por ser persona de alto riesgo para contraer el virus | 46 | 34 | 53 | 38 | 49 | 18 | 16 | 19 | 14 | 12 | -45 | |||||||||
| Aislamiento por tener síntomas o ser un caso | 31 | 46 | 40 | 14 | 18 | -41 | 8 | |||||||||||||
| Restricciones de viaje | ||||||||||||||||||||
| Restricciones de entrada a extranjeros (China) | 19 | 2 | 10 | 54 | 49 | 30 | -1 | 14 | -46 | 14 | 9 | 9 | ||||||||
| Restricciones de entrada a extranjeros (otros países) | 61 | 59 | 39 | 54 | 49 | 43 | 39 | 27 | 22 | 16 | 15 | 14 | 12 | 9 | ||||||
| Cierre de frontera para tráfico no esencial | 57 | 54 | 51 | 51 | 44 | 26 | 14 | 15 | 13 | 10 | 7 | |||||||||
| Restricciones de viajes internacionales | 54 | 58 | 58 | 54 | 48 | 39 | 38 | 32 | 46 | 25 | 16 | 15 | 9 | |||||||
| Restricciones a viajes aéreos domésticos | 31 | 31 | 54 | 48 | 38 | 41 | 25 | 17 | 14 | 16 | ||||||||||
| Restricciones de cruceros | 36 | 54 | 41 | 40 | 12 | 12 | 6 | |||||||||||||
| Detección y rastreo de casos | ||||||||||||||||||||
| Búsqueda intensiva de casos (En puerto de entrada y en todos los entes territoriales/provincias) | 20 | 21 | 6 | 6 | 19 | 44 | 5 | 8 | -32 | 5 | ||||||||||
| Rastreo de contactos | 20 | 21 | 33 | 6 | 10 | -41 | 10 | |||||||||||||
| Uso de tecnología para detectar casos, rastrear contactos y notificar (ej.., termómetros, drive-through, Apps) | 14 | 14 | 6 | 43 | 47 | 34 | -41 | 15 | ||||||||||||
| Laboratorios o capacidades adicionales | 27 | 34 | 21 | 56 | 44 | 44 | 6 | 5 | 18 | -4 | 15 | |||||||||
| Infraestructura del sistema de salud y recurso humano | ||||||||||||||||||||
| Ampliar la capacidad de camas | 34 | 34 | 46 | 41 | 19 | -1 | 4 | 15 | 6 | |||||||||||
| Habilitar el uso de estadios y otros espacios | 34 | 34 | 46 | 44 | 4 | 14 | 16 | |||||||||||||
| Incrementar los insumos (mascarillas, ventiladores) | 56 | 51 | 40 | 46 | 32 | 2 | 16 | -24 | 7 | 1 | ||||||||||
| Inversión en vacunas e investigación | 28 | 39 | 46 | 46 | 34 | 15 | 6 | |||||||||||||
| Incrementar el personal de atención (voluntarios, estudiantes, jubilados, extranjeros, ayudas humanitarias) | 46 | 44 | 46 | 47 | 19 | -2 | -24 | |||||||||||||
| Entrenamiento para médicos | 22 | 44 | ||||||||||||||||||
| Incentivos (monetarios) para personal de atención | 52 | 47 | 17 | |||||||||||||||||
| Estrategias dirigidas a población en riesgo | ||||||||||||||||||||
| Condiciones especiales para mayores de 70 años o niños | 41 | 45 | 38 | 36 | 12 | 12 | 12 | |||||||||||||
| Medidas especiales para población privada de la libertad | 41 | 18 | 18 | |||||||||||||||||
| Levantar medidas de aislamiento para casos de violencia intrafamiliar | 40 | 17 | ||||||||||||||||||
| Limitar el acceso a centros de atención para personas mayores o para hospitales | 54 | 49 | 46 | 10 | 18 | 12 | ||||||||||||||
| Apoyo Social | ||||||||||||||||||||
| Apoyo directo con recursos económicos (Bonos u otra medida) | 50 | 53 | 51 | 41 | 32 | 48 | 15 | 14 | 18 | |||||||||||
| Alivio tributario o crediticio | 50 | 51 | 41 | 46 | 48 | 48 | 15 | 14 | 12 | 11 | ||||||||||
| Apoyo de alimentación u otros insumos para personas vulnerables | 51 | 45 | 51 | 48 | 15 | 14 | 12 | |||||||||||||
| Medidas de protección laboral o de inquilinos (evitar despidos y desalojos) | 42 | 46 | 46 | 18 | 15 | 17 | ||||||||||||||
| Mejorar las condiciones del pago por enfermedad o de incapacidad | 50 | 41 | 32 | 18 | 3 | |||||||||||||||
| Coordinación de donaciones | 49 | 15 | ||||||||||||||||||
| Participación de ONG | 41 | -347 | ||||||||||||||||||
| Intervenciones para respaldar la producción de bienes y servicios | ||||||||||||||||||||
| Apoyo directo con recursos económicos a empresas | 55 | 63 | 53 | 51 | 46 | 40 | 18 | 15 | 21 | |||||||||||
| Alivio tributarios y crediticios y facilitar préstamos a empresas | 55 | 50 | 53 | 51 | 46 | 47 | 48 | 18 | 15 | 21 | ||||||||||
| Planes económicos | 55 | 51 | 56 | 46 | 48 | 18 | 15 | 21 | ||||||||||||
| Planes de suministro de alimentos y medicamento | 40 | 45 | 15 | 14 | ||||||||||||||||
| Control de precios de venta a medicamentos | 41 | 21 | ||||||||||||||||||
| Información, comunicación y apoyo al distanciamiento social | ||||||||||||||||||||
| Aplicaciones móviles con información | 30 | 6 | 16 | 20 | 4 | -15 | ||||||||||||||
| Reportes diarios en medios | 6 | 53 | 49 | 43 | -24 | -32 | 6 | |||||||||||||
| Campañas educativas | 21 | 42 | 48 | 44 | 30 | 32 | 14 | -24 | -32 | |||||||||||
| Publicación de planes, decretos, recomendaciones en sitios web específicos | 53 | 43 | 38 | 28 | -41 | -32 | -7 | |||||||||||||
| Aumento nacional de la velocidad de internet para todos los usuarios | 17 | |||||||||||||||||||
| Habitar líneas gratuitas de llamadas para nacionales en el exterior | 5 | 14 | 10 | |||||||||||||||||
| Fomentar el tele trabajo o la tele-medicina | 55 | 42 | 38 | 15 | 13 | 8 | ||||||||||||||
Anexo 3.
Anexo 3. Hallazgos claves de los estudios que evaluaron impacto de las intervenciones no farmacológicas.
| Medida no farmacológica | Impacto | Hallazgos |
|---|---|---|
| Combinación de medidas | Alto | Dos estudios de modelamiento (SIR) de la infección COVID-19 establecen que las medidas de prevención y control tempranas y estrictas, como la cuarentena, el distanciamiento social o la suspensión del transporte público, reducen la tasa de contacto y la eficacia de la infección, y por ende son clave para contener el brote. (11) |
| Las medidas no farmacológicas como restricciones de viaje entre ciudades, el distanciamiento social y las reducciones de contacto, así como la detección temprana de casos y los aislamientos, han reducido sustancialmente la transmisión de COVID-19 en China. Se estimó que la detección temprana y el aislamiento de casos previenen más infecciones que las restricciones de viaje y las reducciones de contacto (5 veces versus 2,6 veces), pero las medidas no farmacológicas integradas logran el efecto más fuerte y rápido. (12) | ||
| Sin la implementación de las medidas no farmacológicas, el número de casos de COVID-19 habría aumentado rápidamente en China, con un aumento de 51 veces en Wuhan, un aumento de 92 veces en otras ciudades de Hubei y un aumento de 125 veces en otras provincias. (12) | ||
| Los tiempos de implementación de la intervención también son críticos. El número de casos podría reducirse drásticamente en un 66%, 86% y 95%, respectivamente, si los NPI pudieran llevarse a cabo en una semana, dos semanas y tres semanas antes del momento real en el que se implementó en todo el país. Además, el rango geográfico de las áreas afectadas se reduciría de 308 ciudades a 192, 130 y 61 ciudades, respectivamente. (12) | ||
| En la mayoría de los escenarios, el rastreo de contactos es altamente efectivo y el aislamiento de casos es suficiente para controlar un nuevo brote de COVID-19 en 3 meses. La probabilidad de control disminuye con largos retrasos desde el inicio de los síntomas hasta el aislamiento, se determinan menos casos por rastreo de contacto y aumenta la transmisión antes de los síntomas. (13) | ||
| La efectividad de cualquier intervención aislada puede ser limitada, lo que requiere que se combinen múltiples intervenciones para tener un impacto sustancial en la transmisión. (10) | ||
| Las políticas de mitigación óptimas (que combinan el aislamiento domiciliario de casos sospechosos, la cuarentena domiciliaria de quienes viven en el mismo hogar que los casos sospechosos y el distanciamiento social de los ancianos y otras personas con mayor riesgo de enfermedad grave) podrían reducir la demanda máxima de atención médica y la mortalidad entre 2/3 y la mitad. Sin embargo, la epidemia mitigada resultante probablemente resultaría en cientos de miles de muertes y sistemas de salud colapsados. (10) | ||
| En total, en una epidemia no mitigada, se predicen aproximadamente 510,000 muertes en Gran Bretaña y 2.2 millones en los Estados Unidos, sin tener en cuenta los posibles efectos negativos de los sistemas de salud que se verían colapsados. (10) | ||
| Para una epidemia no controlada, se predice que la demanda de camas de cuidados intensivos se excedería tan pronto como la segunda semana de abril, con un pico de demanda de camas de cuidados intensivos mayor a 30 veces la oferta máxima en ambos países. (10) | ||
| Las ciudades que implementaron cualquier combinación de medidas de control de manera preventiva, antes de descubrir cualquier caso COVID-19, informaron 33.3% (IC 95%: 11.1-44.4%) menos casos confirmados por laboratorio durante la primera semana de un brote (13.0, IC 95%: 7.1-18.8, n = 125), en comparación con las ciudades que comenzaron el control más tarde (20.6 casos, IC 95%: 14.5-26.8, n = 171; diferencia entre grupos, U = 8197 z = -3.4, P <0.01). (14) | ||
| Entre las medidas de control específicas, las ciudades que suspendieron el transporte público dentro de la ciudad y / o cerraron lugares de entretenimiento y prohibieron las reuniones públicas, y lo hicieron antes, informaron menos casos durante la primera semana de sus brotes. (14) | ||
| Aislamiento de casos | Alto | Se estimó que la detección temprana y el aislamiento de casos previenen más infecciones que las restricciones de viaje y las reducciones de contacto (5 veces versus 2,6 veces), pero las medidas no farmacológicas integradas logran el efecto más fuerte y rápido. (12) |
| Detección temprana de casos | Alto | Se estimó que la detección temprana y el aislamiento de casos previenen más infecciones que las restricciones de viaje y las reducciones de contacto (5 veces versus 2,6 veces), pero las medidas no farmacológicas integradas logran el efecto más fuerte y rápido. (12) |
| Rastreo de contactos | Alto | En la mayoría de los escenarios, el rastreo de contactos es altamente efectivo y el aislamiento de casos es suficiente para controlar un nuevo brote de COVID-19 en 3 meses. La probabilidad de control disminuye con largos retrasos desde el inicio de los síntomas hasta el aislamiento, se determinan menos casos por rastreo de contacto y aumenta la transmisión antes de los síntomas. (13) |
| Cuarentena de contactos | Alto | Cuatro estudios de cohortes y 15 estudios de modelamiento de la infección SARS (síndrome respiratorio agudo severo) y MERS (síndrome respiratorio de Medio Oriente) confirman la efectividad de la cuarentena de individuos que han tenido contacto cercano con casos confirmados. (11) |
| Solo tres estudios consideraron la efectividad de la cuarentena en ejemplos hipotéticos que también modelaron la infecciosidad presintomática. Los estudios son consistentes en identificar que la efectividad de la cuarentena depende de manera crítica de la dinámica biológica de la enfermedad infecciosa (por ejemplo, períodos latentes e infecciosos) y la transmisibilidad. Cuando la transmisibilidad es relativamente baja (número reproductivo básico <2.5), la cuarentena puede controlar una enfermedad, incluso cuando la infecciosidad precede a los síntomas por varios días. Cuando la transmisibilidad es alta y los síntomas surgen mucho después de la infecciosidad, la cuarentena será insuficiente. (11) | ||
| La evidencia relacionada con las pandemias de gripe indica que la cuarentena de personas expuestas puede retrasar el pico de epidemias locales durante las primeras etapas de una epidemia, lo que ayuda a reducir la carga de la enfermedad y retrasar la propagación. ECDC. | ||
| Una cuarentena de 14 días se considera suficiente para controlar a las personas que han tenido contacto con los casos de COVID-19. La identificación rápida de casos aumenta la efectividad de las medidas de cuarentena. (15) | ||
| Suspensión del transporte público | Alto | En Wuhan, de no haberse establecido ninguna restricción de viaje el 23 de enero, los casos podrían haber aumentado 118% (91%-172%), lo que implicaría haber tenido 13,857 más casos (10,920-20,574), si la prohibición se hubiera decretado tres días antes, se habrían reducido los casos en 47% (26%-58%), lo que implicaría haber tenido 3,103 casos menos (1,732-3,820), los casos se habrían reducido en un 83% (78%-89%) si la medida se hubiera tomado una semana antes. (16) |
| Cancelación de grandes reuniones | Alto | Los datos procedentes de modelos de influenza estacional y pandémica indican que, durante la fase de mitigación, las cancelaciones de reuniones masivas antes del pico de epidemias o pandemias pueden reducir la transmisión del virus. (15) |
| Una revisión sistemática de 24 estudios encontró evidencia escasa pero consistente en que la transmisión de la influenza ocurre entre los peregrinos en los principales eventos religiosos. Los principales eventos deportivos como los Juegos Olímpicos y la Copa Mundial de fútbol detectaron un aumento marginal de la incidencia de todas las enfermedades infecciosas, incluida la gripe, con infecciones principalmente limitadas a los competidores y al personal, en lugar de las multitudes que asisten o la comunidad en general. (17) | ||
| Sostenimiento de medidas de distanciamiento (al menos seis meses después del brote) | Alto | Si el contacto con la población se reanuda a los niveles normales observados en años anteriores, el levantamiento de las restricciones de viaje podría hacer que la epidemia vuelva a aumentar. Por lo tanto, la intervención de distanciamiento social debe continuarse durante varios meses. (12) |
| El principal desafío de la supresión es que este tipo de paquete de intervención intensiva, o algo equivalente, eficaz para reducir la transmisión, deberá mantenerse hasta que esté disponible una vacuna (potencialmente 18 meses o más), dado que se predice que la transmisión se recuperará rápidamente si las intervenciones son relajadas. (10) | ||
| Autoaislamiento de personas sintomáticas | Moderado-alto | El autoaislamiento de individuos con síntomas de infección respiratoria es una de las medidas más importantes para reducir la transmisión de enfermedades y limitar la propagación del virus en la comunidad durante una epidemia. (15) |
| Distanciamiento social de los mayores de 70 años | Moderado | Los estudios siempre consideraron la reducción de contacto unido a otras medidas no farmacológicas. (12) |
| Medidas en el lugar de trabajo | Moderado | Las medidas en el lugar de trabajo (horarios de trabajo flexibles / turnos para empleados, teletrabajo, medidas de distanciamiento físico) se recomiendan en personas con enfermedad respiratoria aguda. (15) |
| Distanciamiento social | Bajo-Moderado | Los estudios siempre consideraron el distanciamiento social unido a otras medidas no farmacológicas. (10-12) |
| Restricción de viaje entre ciudades | Bajo-Moderado | La advertencia de no viajar durante una epidemia tiene como objetivo reducir el número de personas infectadas durante un viaje a áreas o países donde la transmisión comunitaria está en curso; reducir el riesgo de importación de los países afectados y reducir las transmisiones entre los viajeros (por ejemplo, en las colas de los aeropuertos o en los aviones). (15) |
| Restricciones de viajes domésticos | Bajo-Moderado | Las restricciones generales de viaje doméstico pueden tener un pequeño impacto positivo en retrasar una epidemia solo si se implementan durante sus primeras etapas. Tales restricciones pueden considerarse solo durante la fase de contención de epidemias de alta gravedad. (15) |
| Si bien no se pudo contener una mayor propagación de COVID-19, las medidas atribuidas al bloqueo en Hubei ayudaron a reducir la velocidad de la infección y a reducir la correlación del tráfico aéreo nacional con los casos de COVID-19 dentro de China. Al interpretar los cambios observados en el tiempo de duplicación, se deben considerar todas las medidas impuestas en Wuhan. Los datos no pueden diferenciar cuáles de las medidas estrictas tuvieron más éxito, puesto que los análisis solo evaluaron la eficacia de la totalidad de las medidas. La totalidad de las medidas fue parcialmente exitosa y ha resultado en una propagación retrasada de COVID-19 en China. (18) | ||
| La prohibición de viajar de Wuhan retrasó el tiempo de llegada de COVID-19 en otras ciudades en un promedio de 2.91 días (IC 95%: 2.54-3.29 días). Más de 130 ciudades, que cubren más de la mitad del área geográfica y la población de China, se beneficiaron de la demora. Este retraso proporcionó tiempo adicional para prepararse para la llegada del COVID-19 a China, pero no habría frenado la transmisión después de que la infección se haya exportado a nuevas ubicaciones desde Wuhan. (14) | ||
| Cierres de escuelas y guarderías (bajo impacto) | Bajo-Moderado | Los cierres proactivos de escuelas y guarderías pueden estar asociado con costos significativos para la sociedad y la economía. Durante la fase de contención, el cierre de escuelas no está justificado. No hay datos que respalden decisiones informadas sobre el cierre proactivo de escuelas en términos de su efectividad anticipada para mitigar la epidemia de COVID-19, debido al nivel desconocido de transmisión de este virus entre los niños. (15) |
| Cuarentena de viajeros provenientes de zona afectada | Bajo | El número de infecciones y muertes evitadas con la cuarentena de viajeros de un país con un brote declarado es sustancialmente menor que la cuarentena de contactos o casos sospechosos. (11) |
| Un estudio de cohorte retrospectivo y tres estudios de modelamiento abordaron la efectividad de la cuarentena para reducir las transmisiones de individuos que viajaron desde regiones con altas tasas de transmisión. Uno de los estudios de cohorte, consideró evidencia del brote de SARS de 2003 en Taiwán. Los resultados del modelo mostraron que en el escenario hipotético en el que nadie hubiera sido puesto en cuarentena después de llegar de una región de alta transmisión, se habrían producido 511 casos adicionales de SARS con 70 muertes adicionales. En la base de datos, se pudieron rastrear 17 casos importados no puestos en cuarentena (casos perdidos y casos anteriores a la implementación de la cuarentena). Si los 17 casos importados no puestos en cuarentena hubieran sido puestos en cuarentena, 280 casos de SARS y 48 muertes podrían haberse evitado. De las más de 95,000 personas en cuarentena, solo dos desarrollaron SARS. Si estos dos individuos no hubieran sido puestos en cuarentena, se habrían producido 29 casos adicionales y cinco muertes. (11) | ||
| Reducción de contacto | Bajo | Los estudios siempre consideraron la reducción de contacto unido a otras medidas no farmacológicas. (12) |
| Cierres de fronteras | Bajo | Según la evidencia de los estudios de modelos, principalmente relacionados con las pandemias de influenza, los cierres de fronteras pueden retrasar la introducción del virus en un país solo si están casi completos y cuando se implementan rápidamente durante las primeras fases, lo cual es factible solo en contextos específicos (por ejemplo, para naciones pequeñas, aisladas e isleñas). Por lo tanto, la evidencia disponible no respalda la recomendación de cierres de fronteras que causarán efectos secundarios significativos y trastornos sociales y económicos. (15) |
| Procedimientos de detección de casos en aeropuertos | Bajo | Aunque algunos casos importados de COVID-19 se han detectado a través de procedimientos de detección de entrada en los aeropuertos de destino, la evidencia disponible de publicaciones revisadas por pares y el trabajo de modelado no publicado realizado en el ECDC sugiere que las medidas de control fronterizo no son efectivas para retrasar o mitigar una pandemia. Esto se debe a la baja sensibilidad de los sistemas utilizados para detectar infecciones levemente sintomáticas y su incapacidad para detectar casos durante el período de incubación. (15) |